Generative AI and Creative Mediums for Youth's Emotion Regulation: An Interview Study with Clinicians
DOI: https://doi.org/10.1145/3772318.3790909
CHI '26: Proceedings of the 2026 CHI Conference on Human Factors in Computing Systems, Barcelona, Spain, April 2026
Emotion regulation (ER) is essential to youth well-being, and cognitive-behavioral therapy (CBT) is an established approach for building ER skills. Clinicians often use creative mediums such as visuals and narratives to support ER through CBT, yet access and personalization remain limited. Generative AI (GenAI) shows promise for addressing these limitations, but its benefits and risks in youth ER remain underexplored, underscoring the need for expert perspectives. We interviewed 20 ER specialists–psychotherapists, art therapists, and psychiatrists–using a GenAI technological probe that generated CBT-based visuals and narratives. Clinicians highlighted GenAI's potential as a “bridge” to help youth concretely identify and express emotions, practice personalized coping skills, and mediate ER conversations between home and clinics. They also cautioned that the vividness and unpredictability of GenAI outputs may trigger trauma or reinforce maladaptive thinking. We propose psychologically grounded design implications for GenAI to foster safe, engaging youth ER as a foundation for lifelong well-being.
ACM Reference Format:
Daeun Yoo, Daniela E Munoz Lopez, Xiaotian Daisy Hu, Jason C. Yip, and Katie Davis. 2026. Generative AI and Creative Mediums for Youth's Emotion Regulation: An Interview Study with Clinicians. In Proceedings of the 2026 CHI Conference on Human Factors in Computing Systems (CHI '26), April 13--17, 2026, Barcelona, Spain. ACM, New York, NY, USA 18 Pages. https://doi.org/10.1145/3772318.3790909
1 Introduction
Emotion regulation (ER) is a fundamental skill that is linked to psychological well-being and resilience across the lifespan [45, 60], involving the monitoring, evaluation, and management of one's emotional experiences [48]. Childhood is a particularly important period for ER development. As youth mature, they understand and express more complex emotions within an increasing variety of social contexts. Upon entering adolescence, they often experience heightened emotional fluctuations [28, 101, 121, 156]. Without developing adaptive ER strategies to cope with their changing emotions, children and adolescents face elevated risks for depression, anxiety, and aggressive behaviors [5, 89]. Presently, 41.5% of U.S. teens report lacking needed social-emotional support [155], while 40% experience persistent sadness or hopelessness, and 20% have seriously considered suicide [23]. These statistics underscore the need for accessible, engaging, and effective ER support.
Cognitive Behavioral Therapy (CBT) is an established, evidence-based method for building ER skills in both adult and youth populations [10, 83]. CBT has been shown to be effective in treating anxiety and depression among clinical populations [70, 123], as well as adaptable for broader ER skill-building in non-clinical populations [129]. Many core CBT techniques, such as cognitive restructuring, support ER by reducing emotional intensity and fostering adaptive responses [49]. However, several barriers limit the accessibility of these techniques for youth. Clinic-based CBT can be difficult to initiate and sustain due to scheduling constraints and children's reluctance to engage [63, 132]. Self-guided workbooks, used outside therapy for ER practice, often fail to match youth's developmental preferences or sustain their interest [72, 108].
To address these challenges, some clinicians integrate creative mediums, such as visual imagery and storytelling, into their CBT practice with children and adolescents [25, 132, 135]. Visuals such as feelings wheels, which show a diverse set of emotions through color, and drawings can help children externalize their emotions in concrete and richer ways [47, 86, 133]. Narratives such as metaphorical stories and imaginative description can help children identify their emotions and adopt new perspectives [15, 72, 96]. Evidence suggests that these approaches can increase engagement and improve outcomes among children and adolescents [25, 31]. Still, such creative-oriented CBT integrations remain limited, with a need for more transferable guidelines and interactive tools that consistently support both in-session work with clinicians and self-directed at-home practice [84, 96, 143]. Moreover, as long as they remain in analog form, visual and narrative approaches are limited in accessibility and personalization.
There is growing interest among mental health practitioners and researchers in using Generative AI (GenAI) tools to supplement traditional mental health treatments [93], and many teens are interested in using general-purpose GenAI systems (e.g., ChatGPT, Character.AI) for emotional conversations [29, 113]. While GenAI offers new opportunities to deliver personalized and accessible ER support for children and adolescents, such as generating contextually relevant, personalized images and story-based text for youth [12, 32, 100, 111], its growing integration into therapeutic and creative processes [65, 84, 157] calls for critical reflection. Before designing and deploying GenAI tools for youth ER, it is essential to examine both their potential benefits and risks. Without this understanding, youth may be vulnerable to negative outcomes associated with AI interactions, such as self-harm or aggressive behavior [4, 105].
We collaborated with pediatric clinical psychologists to investigate clinicians’ perspectives on using GenAI in youth's ER. This study is guided by the following research questions:
- RQ1: How do clinicians use visual and narrative mediums for youth ER, and what challenges point to opportunities for GenAI support?
- RQ2: What are clinicians’ perceptions and expectations for using AI-generated visuals and narratives to support youth's ER?
We conducted semi-structured interviews with 20 pediatric clinicians, including psychotherapists, art therapists, and psychiatrists, to capture insights from both traditional CBT-oriented and creativity-centered therapeutic approaches to ER skill development. Participating clinicians worked with children and adolescents in their practice; we refer to these populations collectively as "youth" throughout this paper. In this study, we interviewed clinicians rather than youth or caregivers to assess potential benefits and risks before direct use, aligning with HCI work that begins with expert interviews for sensitive or vulnerable populations [81, 152]. This exploratory study examines whether GenAI-supported ER through visual and narrative creation is appropriate for diverse youth populations. To support these interviews, we developed a GenAI-powered technological probe based on Gross's extended process model of ER [90], enabling clinicians to concretely explore how visual and narrative interactions might guide youth's emotional exploration.
Our analysis identified four key findings:
- Current practices: Clinicians use visuals and narratives to scaffold ER through CBT, but face barriers engaging youth due to their varied expressive abilities and the limited interactivity of worksheets.
- Opportunities for GenAI to support youth ER: Clinicians envisioned that GenAI's visual and narrative creation abilities could make ER more accessible and enable vivid, personalized coping-skill practice in clinics and homes.
- Risks of GenAI in ER: The unpredictability of GenAI outputs risks triggering trauma or reinforcing maladaptive thinking, risks exacerbated by the vividness of AI-generated imagery.
- Recommendations: Adapt GenAI to individual symptoms, and ensure clinician and caregiver involvement when used for ER support. GenAI may be helpful for neurodivergent youth or those internalizing feelings, but not for youth experiencing depression or paranoia.
This study contributes empirical evidence on pediatric clinicians’ perceptions of GenAI-assisted tools that leverage visual and narrative creation, highlighting both the areas where GenAI can support youth ER and the risks involved. These insights are time-sensitive and critical to consider as GenAI is increasingly being designed for and used to provide mental health support [54, 84, 157]. In addition, we propose design guidelines grounded in psychological theories for future creative activity–based GenAI tools to support youth's ER development.
2 Related Work
2.1 Supporting Emotion Regulation in Childhood and Adolescence
Emotion regulation (ER) refers to the cognitive processes of monitoring, evaluating, and managing how one responds to an emotionally salient situation [45, 60]. Gross's extended process model of emotion regulation identifies three ER stages: identification, in which individuals identify and evaluate an emotion and decide whether to regulate it; strategy selection, in which they choose an ER strategy (e.g., modify or change the situation, distract oneself, reappraise the situation), and implementation, which involves applying the selected strategy [49]. Challenges at any one of these stages, such as the inability to recognize one's emotions at the identification stage, can lead to ER challenges.
Youth (childhood and adolescence) are critical periods for the development of ER. Children's ability to manage their emotions evolves alongside cognitive, social, and biological changes. By the preschool years, children begin to modulate emotional expressions depending on context. In middle childhood (6-12 years), these expressions become more frequent and influenced by peer and parent relationships [28, 156]. During early adolescence (13–17 years) and late adolescence (18–21 years), youth show greater emotional fluctuations and higher negative mood than children or adults, making it critical to identify potential mental health concerns and provide timely support [101, 121]. Learning adaptive ER strategies is essential, as such skills are closely linked to mental health and life satisfaction [3]. Conversely, maladaptive ER strategies, such as chronic suppression of emotion, increase the risk for depression and anxiety [5, 89].
To support youth's ER, evidence-based approaches such as cognitive behavioral therapy (CBT) [9] and social-emotional learning (SEL) [149] are widely used. SEL curricula foster affective, cognitive, and behavioral skills in school settings and share core practices with CBT [78, 161]. For example, programs like RULER (Recognizing, Understanding, Labeling, Expressing, and Regulating emotions) are designed to promote emotional awareness and regulation in educational contexts [18, 57]. While SEL fosters social and emotional growth in schools, our study focuses on CBT, which more directly addresses individualized needs through short-term, skill-based strategies that help youth adaptively evaluate and modify their thoughts, behaviors, and emotions [11]. CBT techniques, such as cognitive restructuring, support ER by reducing negative emotional intensity, fostering adaptive responses, and promoting acceptance of distressing emotions [49]. Through structured cognitive frameworks and coping strategies, CBT enhances youth's ability to understand and regulate their emotions, and has demonstrated effectiveness in treating and preventing anxiety and related disorders [119, 123, 137].
Despite their effectiveness, these therapies face barriers to implementation with children and adolescents. In clinical settings, clinicians struggle to initiate and sustain participation; families often fail to recognize the need for intervention before symptoms worsen, and youth are often reluctant to engage in the therapeutic process [72, 132]. Even when therapy is initiated, maintaining engagement over time can be difficult due to both practical barriers (e.g., scheduling conflicts) and psychological ones (e.g., therapy fatigue) [63].
To reduce this burden and accommodate youth's individual needs, many clinicians adopt flexible and creative strategies [69]. Similar challenges exist with self-guided CBT workbooks, whose traditional print formats may not always resonate with youth [72, 108]. To address these challenges, child-friendly adaptations have been developed, incorporating image-based worksheets and mood-tracking tools to make ER practices more engaging [46, 135]. However, the effectiveness of ER methods varies depending on a child's symptoms, age, and cultural background [8, 160].
As such, while it is important to provide youth with opportunities to become aware of and express their emotional states, there remains a need for the development of engaging, developmentally appropriate ER tools for use in both clinical contexts and at-home practice [72].
2.2 Using Creative Activities to Support Youth's ER
To enhance youth's engagement in psychoeducation and therapy, therapists flexibly adapt interventions to individual needs, often incorporating creative methods such as storytelling, colorful drawings, playful games, and hands-on activities [26, 43, 72]. Among these approaches, the use of visual art can be particularly effective for teaching and practicing ER, as it helps youth externalize inner experiences [86]. Researchers have found that visuals help youth identify their thoughts and articulate their feelings; children who draw and describe their emotions report more than twice as much information as those who only verbalize [47]. In children and adolescents, coloring mandalas (complex geometric patterns) have been shown to reduce anxiety [31], and weekly art sessions for adolescents with anxiety and depression improved psychological well-being and flexibility through activities such as “Your mind as a metaphor art activity,” where participants created visual representations of their minds [25]. More broadly, there is evidence that visual interventions can reduce anxiety and depressive symptoms across diverse populations, including cancer patients, individuals with depression, and people with PTSD [7, 27, 133].
Compared to verbal thought alone, mental imagery, such as vividly imagining events like a movie in one's mind's eye using the senses, can evoke stronger emotional and cognitive responses [88]. This heightened impact stems from mental imagery's ability to activate brain systems responsive to sensory signals and access emotional memories [58]. Similarly, externally presented visuals can amplify emotional engagement more than verbal stimuli, as visual content often elicits greater emotional resonance. For instance, voluntary visual attention has been shown to increase perceived emotional intensity [98]. Thus, visuals, whether internally imagined or externally presented, could both support ER or inadvertently intensify distress, depending on how they are used.
Complementing visuals, stories and narratives provide another creative pathway for ER support, particularly within CBT frameworks. They help youth adopt new attitudes and beliefs through cognitive reframing, as children derive social and emotional meaning from the narratives [37, 96]. For example, clinicians can use metaphors, such as frogs to illustrate the risks of inflexibility [15], or guide youth to imagine safe locations for relaxation exercises [72]. In clinical interventions, bibliotherapy, which involves the use of narratives to help youth identify and reflect on their thoughts and emotions [80], has shown efficacy in reducing depression and improving CBT completion rates [122]. Creative bibliotherapy applies fictional stories and poetry as a medium for psychoeducation, where selecting age- and literacy-appropriate narratives is essential [96].
This body of work provides a useful foundation for understanding how visuals and narratives support self-expression and ER practice. However, little is known about how well these creative strategies are actually used in youth's ER practice in clinics and at home, and what challenges limit their effectiveness in supporting youth ER.
2.3 Using Technologies to Enhance Creative Methods of ER Support
HCI researchers have examined how interactive technologies such as mobile games [116], Virtual Reality [73, 85, 148], interactive tangible devices [33, 40, 82, 99, 142, 144], personalized breathing guidance and heuristics [94, 146], and AI-based tools [125, 136, 158] support ER in creative ways. Many of these systems make use of rich visual elements to enhance interactivity, personalization, and engagement. Examples include mobile apps that visualize therapeutic progress [145], interactive agents that facilitate art-making [16], and mixed-reality experiences that use immersive scenes to scaffold breathing, grounding, or cognitive reappraisal [64, 74, 131]. Across this work, several design insights emerge. Kitson et al. highlight that design elements and mechanisms that create immersive and vivid sensory experiences can scaffold ER skill development [74]. ARCADIA, a gamified mixed reality system, suggests that ER supportive tools should provide simple interfaces and allow users to guide their own experience [131]. The Emotion Translator, a visual system for representing personalized emotion taxonomies, also show that visual representations can support social and emotional understanding [162].
Narrative-based approaches also offer design insights for how digital systems can scaffold emotional reflection. AI-based tools encourage children to share their emotions and contextual experiences [124], and storytelling systems facilitate shared emotional understanding between youth and adults [117, 147]. Researchers have also explored conversational agents grounded in CBT and DBT methods to deliver psychoeducation and help youth recognize thought patterns [35, 41, 103, 120], while interactive storytelling tools support identifying negative thoughts and exploring alternative perspectives [21, 51, 87]. More recently, LLM-assisted journaling tools have deepened users’ introspection by offering multiple perspectives on their personal experiences [71]. Together, these systems offer design implications for scaffolding ER through conversational and narrative interaction, including engaging approaches to ER skill guidance and self-monitoring [35, 120] as well as concrete examples of supportive chatbot dialogue structures [35].
With the advent of GenAI, researchers are exploring how generative features can make ER interventions more customizable and engaging [54, 92]. Recent work has used GenAI as a co-creative partner in expressive art therapy to lower creative barriers and enhance engagement [36, 84, 163]. Systems like DreamDirector have supported nightmare treatment by improving emotional relief and therapeutic efficiency through AI-generated images and guidance [157]. Other tools, such as DiSandbox, use GenAI to analyze children's emotions during interactions and provide parents with psychological insights to support emotional wellbeing [126]. Despite these promising directions, important gaps remain in understanding technology-supported ER, particularly with GenAI. While some ER skills benefit from adaptive coaching and support for mind–body awareness [75], existing mental health apps often struggle with accessibility and may leave users feeling deceived [67]. Moreover, only few tools are designed specifically for youth, highlighting the need for more youth-centered mental health technologies [34].
Prior HCI work has emphasized the value of immersive experiences, user-directed guidance, personalization, and engaging reflection in technology-supported ER [35, 74, 120, 131, 162]. GenAI systems may extend these benefits by providing adaptive and responsive image and content generation, while at the same time introducing new limitations and risks because their outputs are not fully reliable or controllable [1, 68, 105]. Introducing GenAI into youth ER requires clearer articulation of when GenAI support is appropriate and when it may be unsuitable for safe and effective use , extending prior work examining the roles of technology in children's social-emotional learning support [2]. Although prior studies have examined art therapists’ views on AI-generated art [65] and raised privacy and safety concerns about emotional-support AI [76], little is known about clinicians’ broader expectations, concerns, and safeguards needed for youth-focused GenAI tools. Our study addresses this gap through interviews with pediatric clinicians.
3 Method
3.1 Study Design
We conducted semi-structured interviews with 20 U.S.-based pediatric clinicians to examine their use of visuals and narratives in children's and adolescents’ ER and their perspectives on GenAI for creative ER support. Our multidisciplinary team (HCI, clinical psychology, child development) enabled integration of emotional, developmental, and technical perspectives. The study was approved by our university's Institutional Review Board.
| PID | Role | Treatment Settings | Gender | Years |
|---|---|---|---|---|
| P1 | Art therapist | Private practice | Female | 3–5 |
| P2 | Art therapist (PhD) | Private practice | Female | 10+ |
| P3 | Psychotherapist | Hospital | Female | 5–10 |
| P4 | Psychotherapist | Hospital | Male | 5–10 |
| P5 | Psychotherapist | Hospital | Female | 5–10 |
| P6 | Psychologist (PhD) | Hospital | Female | 5–10 |
| P7 | Art therapist (PhD) | University | Male | 10+ |
| P8 | Student therapist | Hospital | Female | 3–5 |
| P9 | Psychologist (PsyD) | University | Female | 10+ |
| P10 | Art therapist | Private practice | Female | 5–10 |
| P11 | Art therapist (PhD) | Private practice | Female | 5–10 |
| P12 | Art therapist | Hospital | Female | 3–5 |
| P13 | Psychologist (PhD) | Hospital | Female | 10+ |
| P14 | Psychotherapist | Hospital | Nonbinary | 5–10 |
| P15 | Psychiatrist (MD) | Hospital | Female | 5–10 |
| P16 | Psychologist (PhD) | University | Female | 10+ |
| P17 | Student therapist | Hospital | Female | 3–5 |
| P18 | Art therapist (PhD) | University | Female | 10+ |
| P19 | Psychologist (PhD) | Private practice | Female | 5–10 |
| P20 | Psychiatrist (MD) | Hospital | Female | 5–10 |
3.2 Participants and Recruitment
Between January and March 2025, we interviewed 20 U.S. based pediatric clinicians, including psychotherapists, art therapists, and psychiatrists. We interviewed clinicians rather than youth or caregivers, as our goal was to first assess potential benefits and risks before introducing such tools to end users. Inclusion criteria required at least three years of professional experience, prior work with children and adolescents in a clinical setting, and current clinical practice.
We categorized participants as follows: “Psychotherapists” (master's in Licensed Mental Health Counseling), “Art Therapists” (master's in Art Therapy and Licensed Professional Counseling, or PhD in Art Therapy), “Psychologists” (PhD in Psychology or PsyD), “Psychiatrists” (MDs specializing in psychiatry), and “Student Therapists” (PhD students in Clinical Psychology). We balanced the sample between art therapists (N=7) and non–art-based psychotherapists and psychologists (N=13), as these groups bring complementary perspectives to emotion regulation: art therapists often have greater experience with creative mediums, whereas talk-based clinicians typically employ conversation-centered approaches. We also included two psychiatrists to capture perspectives on more severe mental health cases. To ensure a range of perspectives, our sample included clinicians working in hospitals (N=11), private practice (N=5), and university or academic settings (N=4). This distribution captured perspectives from traditional clinical settings, flexible and exploratory practices, and research-informed approaches. We recruited participants through professional mailing lists and referrals from other interviewees (snowball sampling). All participants provided informed consent prior to participation, and their identities were protected through the use of participants ID in all transcripts and reported findings. Each participant received a $50 Amazon e-gift card as compensation. Participant demographics and professional details are summarized in Table 1.
3.3 Technological Probe
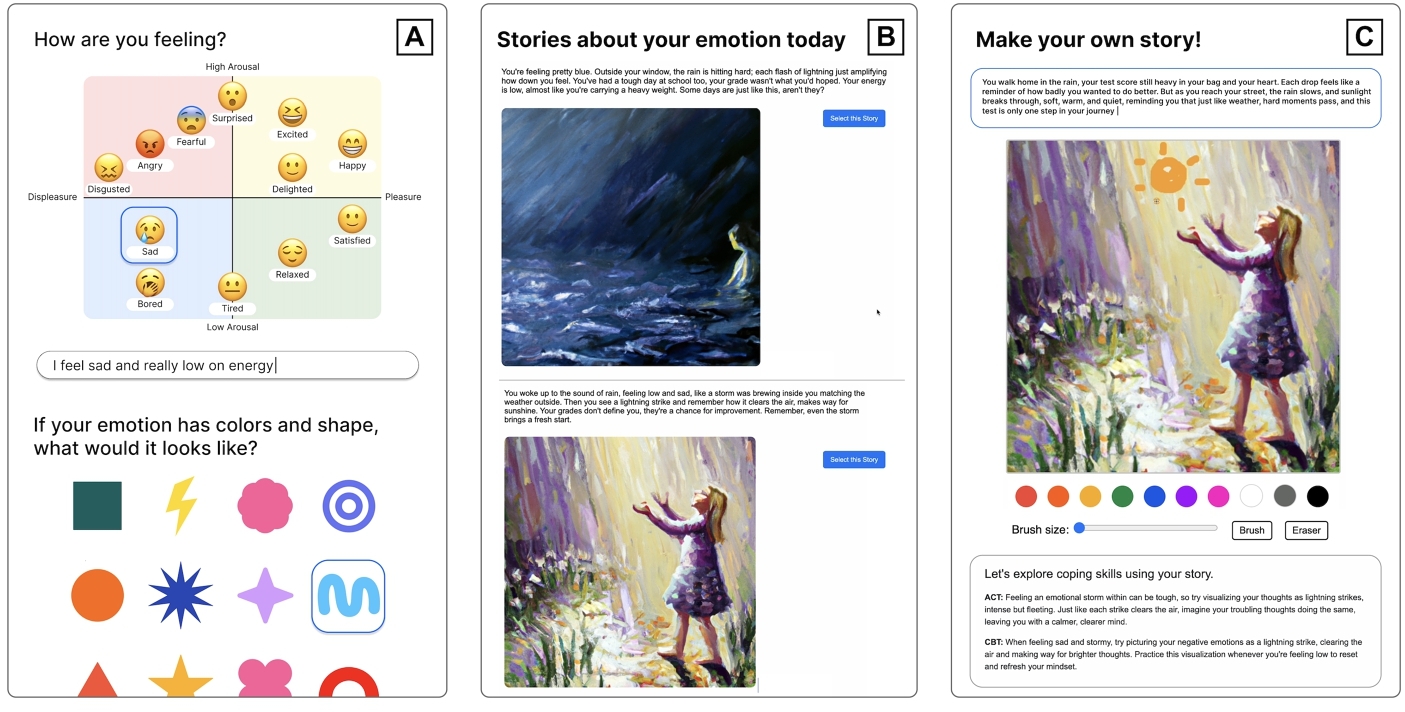
We developed a technological probe (see Fig.1) to give clinicians a clear and direct way to experience how GenAI's creations could be incorporated into youth's ER practice. The purpose of this approach was not to evaluate the probe itself, but to help clinicians identify potential benefits and risks by interacting with it during the interview.
We designed the probe to guide emotional exploration through visual and narrative interactions, drawing on CBT [9] principles that support ER. We used GPT-4 [1] to generate emotion-reflection questions, narratives, and coping suggestions, and DALL·E to produce story-aligned illustrations. We adapted reflection prompts from CBT workbook exercises [108, 135] and structured them to guide users through identifying thoughts, emotions, and behaviors. We configured GPT-4 to implement these prompts by generating age-appropriate, open-ended questions and reflective narratives grounded in users’ inputs.
When designing the interaction flow, we followed Gross's extended process model of emotion regulation [90]: (1) emotional identification, (2) selection of strategies, and (3) strategy implementation. We used this model to design both the screen sequence and guidance content. Gross's model is the most widely cited framework for emotion regulation in psychology and provides a valuable structure for informing design considerations in HCI [128]. Researchers have also used it to demonstrate how CBT techniques correspond to specific ER strategies [102]. We implemented the technological probe in Python and deployed it as a web application on the Vercel platform1 for cross-device access. Each session lasted approximately 10–20 minutes. The following is an overview of the probe:
(1) Emotion identification:In Screen A (Fig.1A), the system guides users through five emotion-related prompts combining text and visuals (emoji icons, colors, abstract shapes). The first three prompts use metaphors such as mood meters, shapes, and weather; later prompts adapt dynamically to earlier responses. A brief validation message concludes the identification stage and invites users to explore their emotions through AI-generated stories and illustrations.
(2) Strategy selection:In Screen B (Fig.1B), the system generates illustrated narratives corresponding to two evidence-based ER strategies: acceptance [53] and cognitive reappraisal [22], based on user input. We chose these strategies because prior research shows they are empirically supported, safe to practice independently, and appropriate for youth [102]. Acceptance guides users to notice and allow emotions without judgment [53], while reappraisal encourages reinterpreting situations to reduce emotional impact [22]. In the technological probe, acceptance appeared through mindful and calming narratives (e.g., “It is okay to feel nervous; we can breathe and let it pass”) with gentle visuals, whereas reappraisal promoted perspective change (e.g., “Maybe this moment can help you learn something new”) through imagery that reframed the situation, such as turning a dark cloudy scene into one with a rainbow. Users then select the strategy that best matches their emotional state and willingness to engage.
(3) Strategy implementation: In Screen C (Fig.1C), the system presents a set of interactive coping skills. Users are invited to edit their narrative and image to better reflect their emotional experience, after which the system offers guided coping exercises based on the user-created content (e.g., if a user selects acceptance and adds a tree to the AI-generated image, floating leaves appear to guide a breathing exercise [14]). Because full implementation in real-world contexts extends beyond the system's developmental stage and the scope of this study, we position the probe primarily as supporting early reflection and rehearsal to help prepare users for real-life practice. Actual implementation would occur through user actions after using the system.
By engaging with this probe during the interviews, clinicians could respond to a shared, concrete example, allowing richer and more targeted reflections on opportunities and concerns of GenAI-assisted ER for youth.
3.4 Procedure and Data Collection
We conducted 20 semi-structured interviews with pediatric clinicians online via Zoom, a video conferencing platform. This format ensured accessibility across time and location and allowed clinicians to participate from private, comfortable settings. Each interview lasted approximately 60 minutes and followed three parts: (1) participants described their current practices supporting youth's ER, focusing on visual and narrative mediums; (2) they engaged with our technological probe by assuming the role of a hypothetical child client; and (3) they shared their perceptions and expectations for using GenAI to support youth's ER based on their interactions with the probe. All interviews were audio- and video-recorded with consent, transcribed, and stored in our university's secure cloud storage.
Interviews began with a five-minute introduction and consent review. The first 25 minutes focused on clinicians’ current use of visuals and narratives in sessions with youth and the challenges they encounter (e.g., “How do you use creative mediums in your sessions?”; “What kinds of difficulties do you encounter?”). We revisited clinicians’ current ER practices to provide a grounding reference point for evaluating GenAI, allowing clinicians to anchor their reflections in familiar workflows and assess more clearly which aspects GenAI could support and where it may be unsuitable. In the next phase, participants spent about 10 minutes interacting with our technological probe, a GenAI-based ER tool with creative supports, while imagining themselves as one of their child clients and thinking aloud about how the child might respond. The final 25 minutes centered on GenAI's potential to support ER through creative visual and narrative methods, as well as perceived risks and concerns (e.g., “What benefits or concerns do you see?”; “How might this tool fit into your workflow?”; “Which features would you add or adjust?”). We also asked how the tool could be adapted for youth with diverse symptoms (e.g., ADHD, autism, paranoia, depression, anxiety) and how GenAI might be involved across ER phases, including awareness, identification, expression, and cognitive change.
3.5 Data Analysis
We analyzed our data using reflexive thematic analysis (TA) [19], an iterative process of identifying and interpreting patterns in qualitative data. Over four months, our process involved three iterations of the codebook and six collaborative meetings to establish consensus and identify and refine emerging themes in relation to our research questions.
To familiarize ourselves with the data (phase one), the first author reviewed all interview transcripts, while the other authors each conducted an in-depth review of two. During this stage, each author independently developed an initial codebook informed by their disciplinary perspective. In phase two, we met twice to share and discuss these codes, after which the first author created a collective version of the codebook. All authors then reviewed two additional transcripts, assessing whether the synthesized codebook adequately captured their findings and proposing new codes where needed. These discussions informed a revised version of the codebook, finalized after two further meetings in which all authors reached consensus on code definitions and examples. In phase three, the first author applied the finalized codebook to the full dataset and documented a brief rationale for each code assignment. A secondary coder reviewed all assignments, noting disagreements, which the team discussed until reaching consensus [55, 56]. Following the coding phase, we held three meetings to refine interpretive themes. All authors organized codes into higher-level categories (e.g., benefits of AI-assisted visuals/narratives, potential use cases of GenAI in ER) through affinity diagramming [52] in Miro,2 an online whiteboard platform.
4 Findings
4.1 Supporting Youth's Emotion Regulation through Creative Activities
Clinicians shared how they currently use physical and digital visual-narrative tools to facilitate emotional communication, support youth's emotional awareness and expression, and teach coping skills. However, they also identified gaps in supporting children's ER during and outside sessions with these tools.
4.1.1 How Clinicians Bring Visuals and Narratives into Their Practice. Clinicians described using visuals and narratives to help youth build emotional awareness, express feelings, and practice coping skills. For instance, clinicians use feelings thermometers to support youth's emotional awareness and expression. P9 (psychologist, PsyD) explained that visual tools and scenarios can make abstract emotions more tangible and open up discussion: "I often rely on visual tools, like emotion wheels, or specific scenarios such as writing out a scenario from the week when [a] child had a hard time. We think about it together visually for the kids." Further, clinicians used stories and visuals to scaffold youth's understanding and expression of abstract emotions by representing these emotions in concrete ways. For example, P10 (art therapist) shared that she used the book Ruby's Worry [107] to teach ER skills: “I sometimes bring in a book like Ruby Finds Worries, and use it as an example. If I start with that visual image, I've planted the seed of ‘what does your worry look like if you were going to create it?’”
Clinicians also used digital images, drawing tools, and image-based worksheets, to teach and practice coping skills with youth. For example, P7 (art therapist, PhD) displayed forest-scene images to guide breathing exercises and mindfulness through visual imagery. Clinicians additionally used digital art tools to address youth's individual challenges. P18 (art therapist, PhD) shared that she uses the Jackson Pollock online tool3, which provides a blank canvas with uncontrollable color and brush behavior, to help youth with OCD or anxiety release perfectionistic tendencies: "If I want someone to practice letting go of perfectionism, I use the Jackson Pollock tool. Some kids, especially those with OCD or anxiety, fear making mistakes. These unpredictable tools help them face that discomfort." Beyond clinical settings, clinicians also recommended that parents use multi-sensory approaches at home to reinforce ER coping skills. For instance, several clinicians encouraged families to practice self-soothing techniques through the five senses, including vision, hearing, and touch. P9 (psychologist, PsyD) explained that these multi-sensory strategies can be effective for youth who have stronger visual than auditory skills, especially when emotions are heightened: "A lot of the kids I see have stronger visual than auditory skills,, relying more on visuals when kids are upset." These examples illustrate that clinicians leverage a range of visual and narrative tools to support youth's ER in concrete and accessible ways.
4.1.2 The Gaps in Practice: When Visuals and Narratives Fall Short. While clinicians widely used creative mediums, they noted two key challenges: (1) youth's varying abilities to express emotions through visuals and narratives, and (2) the limited interactivity and customization of traditional worksheets.
First, not all children and adolescents respond equally well to the same type of visual guidance or expression, since each child possesses different levels of cognitive processing and emotional understanding. For example, youth with ADHD or autism often require more concrete and engaging support than neurotypical youth. P17 (student therapist) explained: “[Neurodivergent kids] need a lot of concrete thinking, so clinicians have to be more creative in how they convey these ideas without relying on abstract comparisons.” She added that analogies, such as describing anxiety as a smoke alarm, often fail to resonate with neurodivergent children. This aligned with P1 (art therapist)’s comment that, although she tailors visual and narrative metaphors to each child's symptoms, doing so requires substantial effort: "I design my stuff and adapt it for each kid… I tend to have a lot of kids with ADHD or ADD, and they get distracted easily."
Additionally, clinicians noted that traditional worksheets lack diversity and interactivity, making it difficult to sustain engagement. P14 (psychotherapist) shared: “I think a traditional worksheet is hard for them to use because they see it so much in hospitals, doctors’ offices, therapists. They get bored or stop taking it seriously.” The repetitive use of the same worksheet over time could reduce its effectiveness. This effect might be especially strong for children with autism, who need continuously updated reinforcers. As P16 (psychologist, PhD) explained: "Children with autism have restricted interests, but those interests and what we find reinforcing can change. Someone might respond well to a sticker chart, but later it's no longer reinforcing. You need to find a new reinforcer." For self-practice at home, clinicians shared that worksheets should include more interactive features, like feedback loops for families. P20 (psychiatrist, MD) noted: "I think parents would feel more confident about some of the resources and handouts if troubleshooting was built into it." These findings illustrate that adding interactivity and personalization to worksheets holds promise for making them more engaging and effective.
4.2 Perceived Benefits of GenAI-Assisted Visuals and Narratives in ER
4.2.1 Accessible Emotional Awareness and Expression. Clinicians envisioned that GenAI-generated visuals and narratives could make abstract feelings more vivid and relatable, helping children identify, express, and communicate emotions with greater autonomy and reduced psychological barriers. After using our technological probe, they emphasized that AI's creations could support youth in identifying and expressing emotions through assisted visualization. For example, P8 (student therapist) noted that GenAI could help children “see their emotions almost come to life and visualize them a bit more.” Similarly, P11 (art therapist) highlighted AI's potential to support youth in externalizing emotions through visual and narrative metaphors: "There's something powerful about a client saying, ’I'm feeling this way: I picture it as a desert with a hyena, a butterfly, and a thunderstorm.’ AI could generate that image for therapeutic use. It's different from drawing by hand, but still meaningful."
Clinicians highlighted AI's ability to generate varied forms, such as colors and weather elements, to represent different types and intensities of emotions based on youth's descriptions. They noted that it could be especially helpful for children with limited skills in identifying and expressing emotions. As P16 (psychologist, PhD) shared: “It gives children different ways to express themselves. It presents visuals in a variety of forms, which I think supports things like emotion identification.” AI's diverse content creation could represent different intensities of the same emotion. For example, rather than showing sadness as a single “rainy day,” AI could create “heavy rain,” “light rain,” or “a rainbow after the rain,” linked to children's experiences. After seeing such variations for the prompt "I'm sad, I feel like a rainy day", P19 (psychologist, PhD) shared that AI's diverse creation could help youth express a range of emotional intensities and qualities: “I think the weather one is great for helping them understand how an emotion might show up differently. When they feel angry, it doesn't always look the same way, they feel it at different intensities and with different qualities.”
Additionally, identifying and expressing emotions through GenAI could serve as a self-directed entry point for youth who struggle with emotional expression through traditional methods, such as paper and crayon. This could be due to difficulties in receiving scaffolding that supports their agency while teaching diverse ways of visualizing emotions. Clinicians envisioned that GenAI could reduce the psychological pressure of expression while providing more autonomy. For example, P12 (art therapist) sometimes gave directive starting points to children overwhelmed by a blank page, while being careful not to provide “too much directive input.” She envisioned that AI-generated visuals and narratives, grounded in children's emotional reflections, could serve as a more "autonomous starting point on their own". This autonomy could be particularly important for youth whose feelings had been suppressed by authority figures, such as parents who avoided emotional discussions. Clinicians noted that GenAI could provide emotional freedom to better identify and express authentic feelings. After using the technological probe, P11 (art therapist) appreciated the feature allowing youth to edit AI-generated illustrated stories which were based on acceptance, cognitive reappraisal, or fact-based approaches:“I love being able to restate what AI brings up. For people who are more depressive or repeatedly criticized, this rewrite narratives and drawing can help them better identify their authentic feelings.” They also emphasized that GenAI-assisted creative expression could mediate emotional communication, especially for adolescents who tend to internalize symptoms. For example, P17 (student therapist) shared: "For adolescents, especially those with more internalizing symptoms, like feeling really sad or afraid without the urge to throw things, communicating through this [the technological probe] could be helpful." These examples highlight how GenAI's visuals and narratives could lower psychological barriers and facilitate emotional communication.
4.2.2 Practicing Coping Skills in Concrete and Vivid Ways. Beyond emotional identification and expression, clinicians envisioned GenAI supporting the practice of coping strategies, such as cognitive reappraisal, a core component of CBT that involves reframing negative thoughts into more positive ones. They emphasized that visuals can help make this abstract skill more concrete and understandable for youth. For instance, P7 (art therapist, PhD) proposed:
"Imagine turning gray thoughts into sunny ones. The AI can ask, ’What makes you happy?’ It's good to acknowledge the negative emotion, but you also need to bring in positive energy with an image. If the kid says ice cream, it could generate that image."
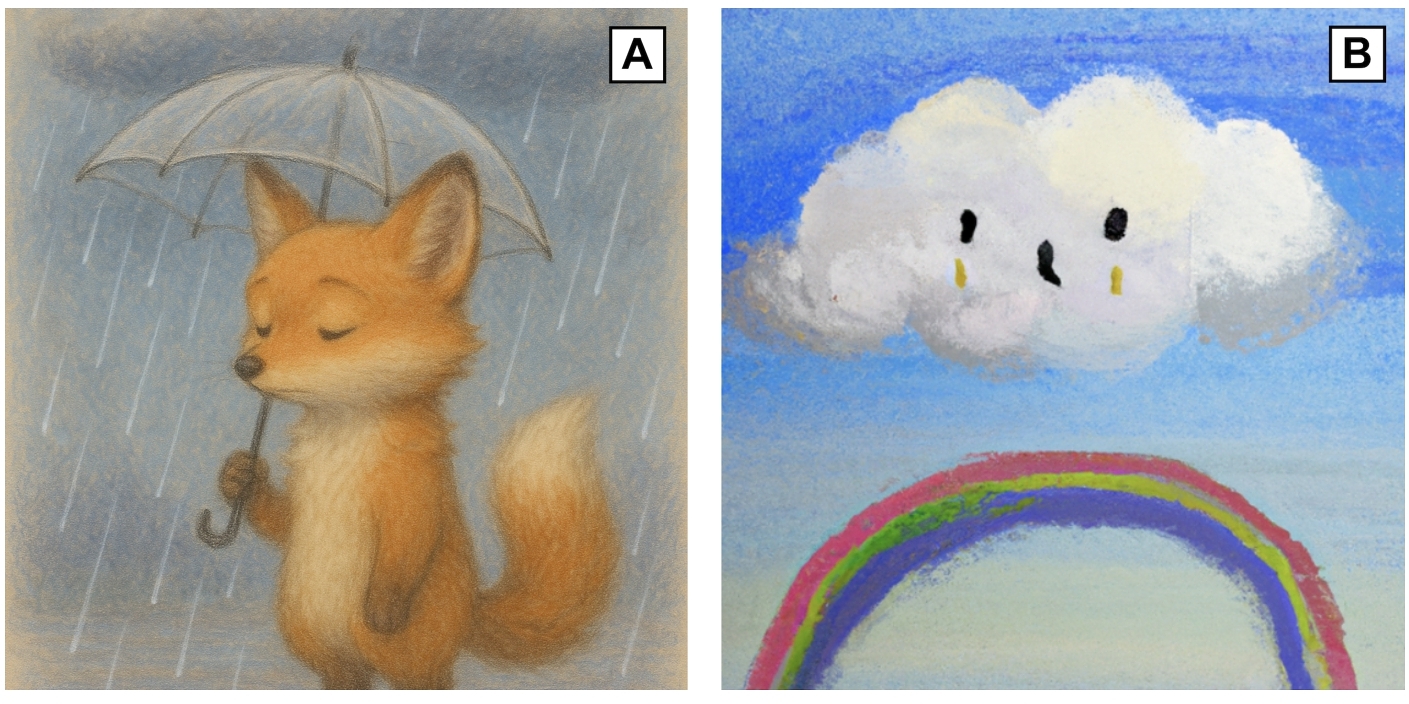
Figure 2 illustrates this positive imagery. For example, if youth drew a fox on a rainy day representing depression (Fig. 2A), GenAI could transform it by adding a rainbow (Fig. 2B). Clinicians also described how GenAI could support clinical interventions through personalized visualizations, particularly for trauma-related symptoms. For instance, P3 (psychotherapist) suggested that for youth with obsessive-compulsive disorder (OCD), AI-generated imagery could scaffold exposure therapy: “For OCD, we use a fear hierarchy and exposure therapy. If a child fears spiders, AI-generated images could help them practice emotion regulation before progressing to real-life exposure..” Some clinicians shared that they had seen colleagues use GenAI to support the rehearsal of coping skills through imaginative storytelling and believed it could be effective. For instance, P19 (psychologist, PhD) shared:
"I've seen people use GenAI to create imaginative stories that let clients rehearse coping skills in advance. The idea is to imagine a situation and practice responding before it happens. That could be really effective."
Clinicians also valued the probe's feature that allowed youth to select from AI's creations and edit them, noting this process could help youth discover coping strategies that best fit their needs. P15 (psychiatrist, MD) highlighted that providing diverse options through AI-generated stories and visuals made coping practice more personally relevant: "I think [AI generated] stories are a really engaging way to teach coping skills. If an adolescent tells you they're feeling bored, you can say the options are either you accept it or you try to change it. Illustrating these two options (ACT / CBT) as a story can help teenagers better visualize the outcome of each route." These reflections highlight GenAI's potential to scaffold youth in finding best-fit coping strategies and to support their practice through concrete visualization.
4.2.3 Creating Personalized, Engaging Experiences. After using our probe, which generates personalized stories and drawings based on youth's conversations with the AI, clinicians shared that youth could find greater relatability and emotional connection in the AI-generated content than in static materials such as paper-based CBT handouts and existing storybooks. They noted that because the stories are rooted in the child's own emotions, the content could feel personal and relevant. As P5 (psychotherapist) shared: “I think this story-writing feels like a creative approach to introduce these skill sets, instead of just a handout. It feels personal, because each of these references ties back to why I was feeling the way I was feeling.” Clinicians saw potential for the content to serve as a shared reference point, supporting collaborative reflection and coping skill practice between youth and adults. For example, P13 (psychologist, PhD) described how an AI-generated story could facilitate parent–child dialogue while viewing an image (Figure 2):
“If the AI creates a story or image of a fox, parents can ask, ‘How does Mr. Fox feel today?’ or ‘What triggers his sadness?’ It becomes an interactive and imaginative way to teach CBT concepts. As they write the story together, they can brainstorm coping skills for Mr. Fox, making the practice more specific and engaging.”
In addition, they valued the flexibility of GenAI to adapt its content based on youth's symptoms, age, and interests. Since effective strategies and triggers vary across individuals and even across different moments, clinicians emphasized the importance of ongoing personalization. For instance, P16 (psychologist, PhD) shared: "For kids whose interests are constantly changing, they might need new ideas to stay engaged. In that sense, GenAI could be helpful, because it can create new content based on what the kid might need."Clinicians also highlighted that GenAI's adaptive visual and narrative support could be particularly helpful for neurodivergent youth, including those with ADHD or autism. P16 (psychologist, PhD) explained: “I recommend different visuals when I'm working with kids with ADHD or autism, because a lot of times they do better with a visual than with words. For neurodiverse and autistic youth, this tool gives options for expressing feelings beyond words.” P20 (psychiatrist, MD) shared: “For youth with mild autism, this tool could be very helpful because they may not naturally communicate visually or verbally. Having different ways to express what they feel and think gives them a more supportive toolkit.” Together, clinicians highlighted that GenAI's adaptable visual outputs may offer youth with diverse cognitive needs more accessible and personalized channels for emotional expression.
4.3 Perceived Limitations of GenAI-Assisted Visuals and Narratives in ER
4.3.1 Unpredictable Outputs and Risks of Maladaptive Distress. Clinicians cautioned that the vividness of AI-generated visuals and narratives, combined with their unpredictability, could trigger trauma or reinforce maladaptive thinking in some youth. They noted that GenAI's unpredictability could produce distressing content that is hard to manage. For instance, P3 (psychotherapist) shared: "We cannot control [GenAI's] output, and it might not know all the ins and outs of patient care. So we don't know what content the child will access." They further cautioned that AI's visual and narrative creations could exacerbate youth's maladaptive thinking. As P4 (psychotherapist) noted:
"If AI's image or story creation unintentionally validates cognitive distortions, especially with paranoia, personality disorders, or long-untreated trauma, that's particularly hard."
P1 (art therapist) also warned that GenAI could intensify paranoid reactions: "I've had clients with severe paranoia, and [ER with GenAI] might not help them. They might say things like, ’This AI is going to destroy my life.’ Clients with highly distorted thoughts might not be good candidates for this."
To mitigate these risks, clinicians stressed the need for contextual and symptom-specific safeguards and active human involvement. P6 (psychologist, PhD) emphasized the risk of repeatedly prompting youth to explore emotions without adequate clinician support, noting that “Youth with depression may be at risk without appropriate support from a clinical professional. Some of the emotions they're working on could potentially trigger suicidal thoughts or even homicidal behaviors.” This highlights that using GenAI with youth experiencing depression or suicidal ideation could be unsafe. They emphasized that therapist supervision enables safe use of AI-generated art and stories. As P7 (art therapist, PhD) explained: "If you have a skilled therapist, they can guide and help reinforce the image in different ways, not just whatever this AI generated. Children need a skilled therapist that's going to take it a little further." These reflections highlight that GenAI's vivid but unpredictable outputs, when used without contextual awareness or human supervision, risk intensifying maladaptive distress.
4.3.2 Misinterpretation Between AI and Youth's Creations. Clinicians observed that the visuals and narratives generated by our probe were often metaphor-based, requiring interpretation by both the child and the AI. They noted that this openness to interpretation could introduce risks if either party misinterprets the other's intent. For example, youth may misunderstand GenAI's image- and narrative-based suggestions if they lack foundational knowledge about emotional concepts, which could lead to inappropriate responses. As P5 (psychotherapist) explained:
"Make sure that the [visual and narrative] outputs feel useful and safe, and that a patient doesn't misinterpret it. If they don't have background knowledge about ‘riding the wave’, which means sitting with an emotion and letting it pass, they might think it means acting on anger or impulsivity instead."
This observation highlights how metaphorical representations, such as describing an emotion as a “wave”, pose a risk of misinterpretation and may hinder the delivery of adaptive psychoeducation.
Conversely, GenAI's own assumptions about metaphor interpretation can also be problematic, since symbols carry different meanings for different people. P7 (art therapist, PhD) described: “The assumption that a partly cloudy day isn't positive is not correct for me. Symbols are subjective, not objective. Maybe in the AI world, a cloudy day means sad or unhappy, but for me, partly cloudy feels relaxing. Fully sunny makes me feel overwhelmed.” These insights highlight the need to balance the expressive flexibility of metaphor with clinically appropriate interpretation, ensuring that meaning is both safe and contextually accurate.
4.3.3 Failure to Detect Red Flag Symptoms. Clinicians in our study expressed concern that GenAI, particularly when generating or interpreting content through visual and narrative mediums, may fail to detect red-flag symptoms such as suicidal thoughts or self-harm intentions. For instance, P4 (psychotherapist) expressed skepticism about GenAI's reliability and emphasized that training it is like training human experts, which requires extensive data and carries inherent risks: "GenAI is trained on a set of data, influenced by what it learns, just like training new therapists. We accept some risk with trainees. How much training would an AI need before it's considered low enough risk to act without supervision?" P20 (psychiatrist, MD) similarly questioned AI's capacity to recognize distress signals embedded in youth's creations: "It's hard to know when the AI should continue or redirect. Knowing when to step in or guide is a human skill, and I don't know if AI has that. If using AI is not monitoring youth's creation like suicidal thoughts, that's risky." Clinicians were particularly skeptical of GenAI's ability to interpret metaphorical or ambiguous expressions of distress. P10 (art therapist) noted that even direct language, such as “I want to die,” may not always reflect suicidal intent and must be understood contextually: "The biggest issue that comes to mind is self-harm and suicidal ideation, and how a tool like that could handle triggers or warning signs. For example, if children or teens write, ‘Sometimes I just want to die,’ they don't always mean they want to kill themselves." Interpreting such intentions could become more complex when youth express emotions indirectly through metaphor-based visual or narrative modalities.
4.3.4 Overreliance Without Critical Thinking. Clinicians expressed concern that GenAI's personalized and engaging features may lead youth to become attached to the tool, which could ironically contribute to emotional dysregulation and impulsive behaviors. For example, clinicians noted that GenAI's flexibility and unpredictability in content generation could be risky if youth use it to reinforce maladaptive thinking. As P8 (student therapist) shared: "If there's no barrier to what they can retype or edit, I'd worry that someone could change the AI's creation so much that it ends up reflecting more negative moods." They emphasized that this risk may be greater for youth who lack the critical thinking skills to evaluate GenAI's suggestions. For these users, independent interaction could be unsafe. As P5 (psychotherapist) shared: “I'm hesitant to consider GenAI for someone vulnerable to suggestion without the critical thinking skills to evaluate it.”
GenAI's interactive features, such as conversational natural language processing and use on digital devices, raised concerns that some youth could become overly engaged or even develop addictive patterns of use. For example, P15 (psychiatrist, MD) shared concerns about youth's overattachment through ongoing conversation with Gen AI: "I've heard the horror stories like those children and teenagers who like to talk with AI robots a lot, and then they get attached to them in an unhealthy way." To address these concerns, clinicians recommended integrating control features to prevent overuse or dysregulation, such as limiting screen time. As P10 (art therapist) suggested: "Set limits, such as timers that shut AI tool down." These concerns highlight that GenAI's engaging and responsive visual and narrative content could also lead to unhealthy attachment and overreliance if not carefully managed.
4.4 Clinicians’ Recommendations and Potential Use Cases
4.4.1 Supporting Concrete and Personalized ER. Clinicians recommended that GenAI support personalized ER by creating diverse and descriptive visuals and narratives to foster youth's autonomous emotional expression. They also noted that these features could be especially useful in group sessions where individualized support is limited. They recommended that GenAI provide interactive and descriptive visual and narrative metaphors, helping youth co-create characters and emotional story contexts. P6 (psychologist, PhD) noted: “Having an interactive piece would be really helpful to grab kids’ attention. GenAI could ask about color, shape, or how they want to represent their emotion.” P17 (student therapist) described that descriptive content can make ER safer and more effective: "Some kids really connect with metaphors… a descriptive, realistic narrative is generally safer." Clinicians also emphasized the importance of giving youth visual choices so they can autonomously decide which coping strategies to practice. P9 (psychologist, PsyD) stressed: “GenAI should give some examples of calm thoughts visually. Giving youth the autonomy to select the calm thought or the self-affirming statement they want to use would be helpful.” Clinicians envisioned these concrete and personalized features could support group ER sessions by offering alternative ways for youth to express emotions when individual attention is limited. As P16 (psychologist, PhD) explained: “In group therapy, you usually have to go around and share, which can be hard for some kids. [Expressing with GenAI] can be another way to show what you're feeling.” Similarly, P18 (art therapist, PhD) noted its value in school-based ER sessions, where students could create their own stories and share them with the group.
4.4.2 Adapting to Individual Youth and Involving Adults. Clinicians emphasized the importance of tailoring GenAI-assisted ER to youth's individual needs while balancing autonomy and adult involvement to ensure safety. First, they noted the need for adaptability to youth's symptoms, such as using more interactive and concrete metaphors for neurodivergent youth. As P18 (art therapist, PhD) explained: “Children with autism are not going to understand symbolism or metaphors that AI creates. It's very hard because they're concrete and literal. For kids on the developmental spectrum, something more descriptive and detailed might work better.” Similarly, P14 (psychotherapist) shared: “When I work with neurodiverse youth, it's less talk therapy and more like a game I created. [GenAI] could play that role for them.”
Clinicians also emphasized the importance of involving adults to ensure the safe use of GenAI, explaining that adults can help reframe and interpret unexpected content. For instance, P3 (psychotherapist) suggested:
"If [ER with GenAI] can be done with an adult, that will be helpful. If AI says [risky things] that somehow trigger the child, the adult can work in real time to reframe it."
Adult involvement should vary by age; younger children benefit from more support, while teens value independence. P6 (psychologist, PhD) shared: “Parents should be more supportive and work alongside younger children, but it may be easier for teenagers to work independently.” P15 (psychiatrist, MD) added: “Teenagers may be reluctant to use [GenAI] if it involves parental oversight.” Accordingly, clinicians emphasized the need to balance autonomy and parental involvement. Some features can promote independence, while others should actively involve adults to ensure emotional safety and support. As P3 (psychotherapist) suggested: “Teens should answer questions independently with AI, but an adult can join during generation to process responses together.” These insights underscore the need for both personalized content and flexible adult engagement to support safe and effective GenAI-assisted ER practices.
4.4.3 Continuity of ER Between Home and Clinic. Clinicians envisioned that GenAI-assisted creations could be brought into therapy sessions to support emotional reflection and continuity between home and clinic. If youth engage with GenAI at home and bring in narratives or visuals they created, these artifacts can serve as meaningful entry points for clinical conversations. For instance, P4 (psychotherapist) noted the time-saving and relational benefits of using content created by youth at home: "If the teen accepted this narrative and made it their own, it would definitely save time because we'd have a starting point. If they endorsed a strong emotion, maybe it walks them through it." Similarly, P19 (psychologist, PhD) highlighted how such artifacts could uncover recurring emotional patterns: “Understanding a person's interpretation of a situation can lead to meaningful conversations and help intervene if a thought pattern keeps coming up.” AI-generated visuals could also support interpretation of youth's emotional states and preferred coping styles. As P20 (psychiatrist, MD) explained: “If a child says they were an orange triangle one day and a blue oval another, we can look at that together and ask, ‘What was happening then?’ That kind of specific recall is helpful in CBT, it grounds the conversation and helps us analyze what they were thinking and doing at that time.” These envisioned use cases suggest that AI-generated visual and narrative content can help youth externalize emotions, facilitate reflection, and foster engagement in ER sessions both in clinics and at home.
5 Discussion
Our analysis indicates that GenAI may not always be an appropriate tool for supporting youth's ER; however, when carefully designed, it could offer benefits in specific contexts. Building on prior work in psychology [49, 58, 72, 77, 97] and HCI on supporting youth's ER [39, 61, 128, 129, 153], we organize our discussion into two parts: (1) how clinicians envision GenAI's creative abilities for supporting ER in youth, and (2) design implications for developing GenAI-based tools to foster youth's ER through creative mediums, including recommendations and strategies to minimize risk.
5.1 Clinicians’ Expectations for Using GenAI to Support Youth ER through Creative Means
We identified two key challenges that clinicians regularly face when using visual and narrative tools to support youth's ER: (1) youth's varying abilities to express their emotions through visuals and narratives, and (2) the limited interactivity and customization of traditional therapeutic tools such as practice worksheets. We propose that GenAI may help address these challenges by acting as a “bridge” that supports youth in recognizing and expressing their emotions. GenAI could provide three types of bridging support, extending the capabilities of prior ER technologies in HCI research:
- Emotional and cognitive support, by offering concrete content for understanding emotions and an autonomous starting point for expression.
GenAI enables adaptive, real-time reflection compared to earlier tools such as 3D computer games and mixed reality platforms with predefined options.
- Personal relevance, by generating coping strategies through personalized and interactive formats based on youth's own creations. GenAI creates evolving, personalized metaphors that deepen youth's meaning-making.
- Connections between the clinic and home, by enabling clinicians and youth to co-reflect on emotions and thoughts using AI-assisted artifacts created at home, which can capture rich emotional detail.
5.1.1 Emotional and Cognitive Support. Clinicians emphasized that AI-generated visuals and narratives have the potential to scaffold youth's emotional understanding and expression in accessible and autonomous ways, while reducing the psychological burden of initiating difficult emotional conversations (Section 4.2). Such support can help youth identify maladaptive thought patterns and articulate their emotions [25, 47, 72]. GenAI can expand youth's emotional awareness by offering diverse visualizations of both intensity and quality. For instance, as clinicians suggested in Section 4.2.1, sadness could be represented not only as a ’rainy day’ but also as ’light rain,’ ’heavy rain,’ or even ’a rainbow after the rain.’ Such variations echo traditional ER tools, such as feeling thermometers and wheels [150, 151], but offer richer scaffolding for both identification and nuanced self-expression.
Clinicians also envisioned GenAI reducing the pressure of emotional expression while preserving youth agency. Unlike paper-and-crayon tasks that may overwhelm youth with a blank page or directive prompts, AI-generated content can provide a flexible “autonomous starting point.” Youth can reflect on AI's initial creations and adapt them to represent deeper feelings. This autonomy is particularly important for youth experiencing emotional dysregulation, especially those whose emotions have been suppressed by authority figures or who internalize symptoms [13, 114].
While earlier ER technologies used predefined visuals or rule-based feedback, GenAI further enables dynamic co-creation by generating adaptive images and narratives that evolve with users’ inputs in real time. In doing so, GenAI complements and extends expressive technologies such as 3D computer games [30] and mixed reality platforms [74, 131] through a highly adaptive, responsive interaction that evolves collaboratively with the user.
5.1.2 Personal Relevance. Clinicians saw promise in GenAI's ability to make ER-focused therapy more personalized and engaging by grounding therapeutic content in youth's own creations. They emphasized the use of metaphors and stories that reflect individual youth's emotions and preferences, consistent with prior work focused on using drawing and narrative for emotional exploration [15, 47]. Moreover, clinicians noted that existing ER worksheets often lack relevance and interactivity, leading to disengagement, echoing findings that clinicians struggle to sustain youth engagement even with creative methods [72]. Many existing tools also rely on reading and lecture-style delivery, which reduces youth's and parents’ engagement and participation levels [139, 140]. To address these challenges, clinicians recommended integrating metaphors drawn from youth's everyday experiences (Section 4.2.3), supported by psychological practices showing that child-created drawings and stories can facilitate emotional expression [135, 154]. Clinicians also highlighted the value of interactivity and multisensory feedback, aligning with prior HCI research on interactive and sensory-based systems that support coping strategies through multimodal engagement [95, 104, 141].
Compared to earlier HCI systems that utilized interactivity and multisensory feedback within predefined structures, such as mobile CBT platforms and biofeedback-based ER systems [41, 82], GenAI can adaptively generate contextually resonant stories and visuals from users’ own creations , such as sketches, colors, or reflections. This generative feedback loop can transform user-made content into evolving emotional narratives, supporting collaborative meaning-making and creation of personalized metaphors, a need highlighted in Kitson et al.’s review [75].
5.1.3 Connections Between the Clinic and Home. Clinicians envisioned GenAI as a bridge between clinical treatment and home-based ER support, particularly for youth with diagnosed mental health conditions (Section 4.4.3). CBT emphasizes collaborative goal-setting and emotional monitoring among youth, therapists, and caregivers [135], which is a key factor in youth ER outcomes [110]. However, this process is often difficult in families less open to emotional dialogue [50] or with youth who are reluctant to share their therapeutic experiences at home [91]. In such contexts, AI-generated visuals and narratives may offer a non-confrontational way for youth to express emotions at home. GenAI's ability to generate metaphors and personalized stories parallels CBT techniques that use metaphor to process complex emotions [44, 97], offering an alternative to direct disclosure and supporting communication for individuals with complex needs [79]. Such conversations around AI-created artifacts could help parents and youth practice ER together at home, whether as homework between sessions or through independent ER activities [130, 140].
In addition, GenAI can bridge clinic guidance and home practice by translating clinician concepts into family-friendly, situation specific artifacts (e.g., visual cue cards or a customized reappraisal storybook) tailored to the youth's age and home caregiver. Clinicians can input their own terms or homework goals, and GenAI can draft a simplified home version with everyday examples for clinicians to refine before sharing with families. This extends prior efforts to connect clinical and home practice, such as HCI work using smartphone apps and clinician portals to link home activities with clinic care [127]. GenAI uniquely supports nuanced, artifact-based continuity by generating and iteratively refining context-specific artifacts. Such artifacts can help youth recall emotions and events in greater detail [72], which in turn can enable richer communication with clinicians.
5.2 Design Implications for GenAI in Youth ER
Here, we draw on our findings to propose a set of design implications to ensure the effective and safe integration of GenAI into creative-based ER support for youth. While GenAI's visuals and narratives could support concrete emotional expression and coping strategies, they may also pose risks if the system triggers trauma or maladaptive distress. In such cases, GenAI's vivid outputs could inadvertently exacerbate cognitive or emotional struggles, as mental imagery [58, 88] and external visual stimuli [98] have been shown to evoke stronger responses than verbal thinking. Therefore, GenAI systems for youth ER support should include safeguards and be grounded in clinical evidence to ensure safe use.
We present design implications organized using Gross's extended process model of emotion regulation [49]: emotion identification, strategy selection, and implementation. We also incorporated a fourth stage, monitoring, as proposed by Slovak et al. [128]. For each stage, we link implications to psychological literature and compare GenAI-specific affordances with prior non-GenAI HCI work, clarifying where GenAI aligns with or extends existing ER technologies. We also outline guidance for safe use, emphasizing the distinct roles required of parents and clinicians in GenAI contexts.
These implications are preliminary and require further validation, as they reflect clinicians’ general viewpoints rather than guidance tailored to specific patient groups. Summaries are provided in Table 2 and described in detail in the following sections.
| Emotion identification | Strategy selection | Implementation | Monitoring | |
|---|---|---|---|---|
| Consideration in ER | Awareness of emotion, emotion labeling [77] | Provide strategies considering cognitive and psychological resources, and emotion intensity [49] | Translation of general strategies into situation-specific tactics [49] | Strategy evaluation and adjustment, symptom tracking [128] |
| Design Recommendations for GenAI | Assist emotional understanding by creating interactive and descriptive outputs (e.g., colors, scenes) | Suggest a set of adaptive strategies (e.g., cognitive reappraisal, mindfulness) through relevant creations | Generate coping skills from youth's creations through personalized visuals and narratives | Provide visual histories of thoughts, emotions, and behaviors for reflection (e.g., storybook library). |
| Guidance for Safe Use | Gather full context of the child; pause if red flags are detected | Provide contextually-relevant scenarios with safe, positive strategies | Guide with concise, easy-to-follow creations to prevent confusion | Adults engage in co-reflection and monitor youth's emotional status |
| Clinicians’ and Parents’ Roles | Provide triggers or sensitivities so the AI avoids generating inappropriate content. | Support autonomy by letting youth explore and regenerate AI options to find a better fit. | Support co-construction to ensure safe, clear interpretation of AI content. | Guide co-reflection and help youth adjust how much to share with AI and adults for privacy and safety. |
5.2.1 Emotion Identification. The first phase of Gross's extended process model of emotion regulation is emotion identification, which is the ability to recognize and label one's emotions [49]. Emotion identification is closely tied to emotional awareness, which requires specific vocabulary to explain one's feelings [77]. Since youth are still developing these skills, their limitations can increase risk for internalizing problems [38]. As outlined in Table 2, GenAI's interactive and descriptive outputs (e.g., diverse colors and scenes) could support youth's emotional awareness and understanding. Outputs such as an illustrative story based on a user's day may help youth identify and explore their thoughts, emotions, and behaviors in open-ended ways. This design insight builds on prior HCI systems that supported emotional reflection through mobile apps and emoji-based tools for Autism Spectrum Disorders [39, 62], while extending them through more personalized and contextually responsive visual and narrative prompts for emotion labeling. For safe use, the system should gather key contextual details in case pre-questionnaires miss red-flag symptoms such as suicidal thoughts or paranoid responses. If any red flags are detected, the system should pause use and alert clinicians, as GenAI-supported ER is not recommended for youth with depression or paranoia (see Section 4.3.1). Extending prior HCI work that collects children's content preferences in AI systems [138], parents or clinicians should also provide relevant contextual information or triggers. For instance, if a child with autism is sensitive to sensory overload (e.g., loud noises, flashing lights) [106], parents could record this so the system avoids generating high-intensity or visually inappropriate scenes.
5.2.2 Strategy Selection. The second phase of Gross's ER model, selecting ER strategies, involves evaluating and choosing among options based on cognitive and physiological resources and emotional intensity [49]. Adaptive strategies such as cognitive reappraisal and mindfulness are generally preferable to emotion suppression, though their effectiveness varies by context and age [17, 20]. To support this phase, designers could leverage GenAI to present a variety of adaptive strategies (e.g., cognitive reappraisal, mindfulness) through contextually generated visuals and narratives, rather than emphasizing a single option. For safe use, the system should generate contextually-relevant scenarios based on youth's emotional and behavioral status, offering safe coping options such as positive imagery or physical activity [74, 104]. Since youth with emotion dysregulation or neurodivergent profiles often benefit from having greater autonomy and choice during ER strategy selection [106, 114], parents and clinicians should support flexibility in how they explore options. This may include prompting GenAI to regenerate strategies with more personally relevant images or narratives.
5.2.3 Strategy Implementation. The implementation phase involves translating a selected ER strategy into specific, situation-appropriate tactics [49]. Our findings suggest that GenAI could generate personalized, evidence-based examples of strategy implementation using creative and relatable metaphors (see Section 4.2). Designers could leverage youth's own creations to create interactive practices that feel meaningful to them. For example, if a child depicts sadness as a blue wave, GenAI could animate it into a breathing exercise, adjusting tempo and color to support regulation. While prior HCI work has explored interactive devices such as robots and tangible tools to support coping-skill practice [33, 153], GenAI may complement these approaches by digitally adapting youth-created metaphors into more personalized and contextually responsive regulation practices. To ensure safety, systems should use clear, easy-to-follow visual and narrative creations to guide youth and prevent confusion that could lead to maladaptive coping strategies [135]. For example, instead of vaguely saying “think positively,” the system could scaffold: acknowledge the negative feeling, ask “What does make you happy?”, take the response (e.g., ice cream), and generate a bright image to shift gray thoughts into sunny ones. Lastly, adults should help reduce misinterpretations and reinforce skill practice through co-construction. While prior HCI work has shown that adult–child scaffolding and joint meaning-making are essential for ER practice [109, 130, 140], GenAI further heightens the need for adult involvement. Because GenAI outputs can be misinterpreted or vary in stability, adult co-construction (e.g., “Which part of this suggestion could we reframe together?”) becomes especially important. When guided well, AI-generated drawings and narratives can serve as powerful mediating artifacts that deepen shared reflection between adults and youth.
5.2.4 Monitoring and Adjustment. Monitoring—an HCI-based extension of Gross's ER model—involves deciding whether to continue, stop, or adjust a chosen ER strategy after reflection [128]. Our findings suggest that GenAI could generate visual histories of youth's thoughts, emotions, and behaviors to scaffold this reflection over time. For example, youth's emotions and behaviors could be visualized in age- and symptom-appropriate ways, such as an “emotional storybook library,” aligning with prior HCI work that transformed youth's recorded emotions into storybooks for reflection [115, 159]. This approach echoes Sanches et al.’s call for mental health technologies to rely less on raw tracked data and more on supporting understanding and reflection [118]. For safe use, parents and clinicians should also co-reflect on youth's emotional and behavioral patterns, as highlighted in prior HCI work on collaborative monitoring [24, 66]. With GenAI, it is especially important to consider what youth choose to share and in what form (e.g., direct AI-chat responses or AI-generated metaphorical outputs) to balance privacy with safe ER practice.
5.2.5 When GenAI Should Not Be Used for ER. Clinicians in our study also raised contexts where GenAI-supported ER may require caution or when it should not be used at all. As described in Section 4.3.1, clinicians cautioned that GenAI-supported ER may be unsafe for youth with paranoia or long-untreated trauma, as "AI's image or story creation may unintentionally validate cognitive distortions". They also raised concerns that youth with depression may not be an appropriate fit, noting that reflecting on certain emotions without clinical support "could potentially trigger suicidal thoughts." Based on these concerns, we do not recommend GenAI-supported ER for youth presenting with these symptoms. At the same time, clinicians emphasized that youth without these symptoms may benefit from GenAI-supported ER via its visual and narrative creation, particularly youth with “internalizing symptoms during moments of sadness or fear” (Section 4.2.1) and neurodivergent youth who need “alternative ways to express feelings beyond words” (Section 4.2.3).
However, many youth and families may be unaware of underlying mental health conditions that require clinical support [72]. Future GenAI tools for ER should therefore embed validated screening questionnaires such as PHQ-9 [112], GAD-7 [134], ASQ [59], and PWQ [42]. These can be administered during onboarding and at regular intervals. If screenings flag a user as at-risk (e.g., suicidality, paranoia, trauma indicators), the system should not launch and instead redirect to clinical professionals. Users who do not screen at-risk may proceed with regular re-assessment, ensuring that at-risk youth are routed to supervised care while maintaining safer access for others. Additionally, we recommend that GenAI-based ER tools be used only with the presence of an adult for children ages 6–12, and under adult supervision for adolescents (13–17). We do not recommend use for preschool-aged children (5 years) due to risks such as false memory implantation and distorted recall [105].
6 Limitations and Future Work
First, our interviews were limited to clinicians in the United States. While this single geographic focus provided valuable insights into a specific population and system, it does not capture the perspectives of clinicians globally. Future research should examine how clinicians in other regions of the world approach youth ER and their perceptions of GenAI, particularly in light of systemic and cultural differences [6]. Second, our technological probe was built with OpenAI's ChatGPT-4o and DALL·E. We implemented safeguards (e.g., prompting the models to avoid risky outputs), which functioned adequately in this study. However, because these models are continually updated, future versions may present different risks, and other GenAI models may behave differently, introducing risks not captured in our findings. Future research could therefore examine both opportunities and risks across a range of GenAI systems and their most current versions. Third, the probe used in the current study required user actions during the strategy implementation phase, as it did not actively support coping practice in real world settings. We adopted this approach given the study's exploratory focus, but future work should enable fuller implementation after carefully assessing the risks and opportunities identified here. Fourth, this was a single-session interview study, and clinicians interacted with the probe for only 10–15 minutes, limiting our understanding of how AI-generated visuals and narratives may fit, or fail to fit, within traditional CBT-based ER practices. Future work should deploy such tools in clinical contexts so clinicians can integrate them into therapy sessions or assign them as at-home activities to assess feasibility and appropriateness in practice. Fifth, this study did not directly examine differences across youth subgroups, such as developmental stages or distinct clinical profiles. Given our exploratory aim to understand clinicians’ broad perspectives on GenAI and youth ER, we centered our analysis at a general level. Future work should investigate how GenAI-supported ER may function differently across specific youth groups. Finally, this study did not include youth or caregivers, as we intentionally focused on clinicians first to identify potential benefits and risks before involving youth; as a result, clinicians’ views may not fully reflect youth's lived experience. Future work should engage youth, caregivers, and educators to co-develop feasible, youth-friendly interventions.
7 Conclusion
In this paper, we investigated how clinicians use visual and narrative mediums to support youth's ER, and how they perceive and expect to use GenAI for this purpose. To do so, we formed a multidisciplinary team of HCI researchers and clinical psychologists and interviewed 20 clinicians, including psychotherapists, art therapists, and psychiatrists, using a GenAI technological probe grounded in CBT principles focusing on ER.
We found that GenAI's ability to generate narratives and visuals from customized input expands opportunities for concrete and personalized ER. These non-directive media may also help youth initiate emotional conversations with clinicians and parents. At the same time, clinicians emphasized the need for caution, given GenAI's limited sensitivity to symptoms and risks of misinterpretation through metaphorical content. Based on these insights, we propose design implications for developing safe, engaging GenAI-supported ER tools informed by psychological theory.
We do not envision GenAI diagnosing or fully understanding emotions, but see potential for it to support youth's emotional expression and scaffold ER skills alongside expert clinicians and supportive family members. This study contributes to the HCI community by identifying both the promise and risks of GenAI in youth ER. We call for technologies that harness their strengths and embed safeguards to ensure safe, effective support for youth ER development as a foundation for lifelong mental health.
Acknowledgments
This work was supported in part by the National Science Foundation (Grant Nos. 2314195 and 1941679) and the Spencer Foundation (Grant No. 202400145). Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the funding agencies. We sincerely thank the clinicians who participated and shared invaluable insights that made this work possible. We also thank JungEl Ryu for support and encouragement.
References
- Josh Achiam, Steven Adler, Sandhini Agarwal, Lama Ahmad, Ilge Akkaya, Florencia Leoni Aleman, Diogo Almeida, Janko Altenschmidt, Sam Altman, Shyamal Anadkat, et al. 2023. GPT-4 Technical Report. (2023). arXiv:2303.08774. Retrieved from https://arxiv.org/abs/2303.08774.
- Naseem Ahmadpour, Lian Loke, Carl Gray, Yidan Cao, Chloe Macdonald, and Rebecca Hart. 2023. Understanding how technology can support social-emotional learning of children: a dyadic trauma-informed participatory design with proxies. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems. 1–17. https://doi.org/10.1145/3544548.3581032
- Amelia Aldao, Susan Nolen-Hoeksema, and Susanne Schweizer. 2010. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review 30, 2 (2010), 217–237.
- American Psychological Association. 2025. Using Generic AI Chatbots for Mental Health Support: A Dangerous Trend. APA Services. https://www.apaservices.org/practice/business/technology/artificial-intelligence-chatbots-therapistsAccessed 2025-08-14.
- Ananda Amstadter. 2008. Emotion regulation and anxiety disorders. Journal of Anxiety Disorders 22, 2 (2008), 211–221.
- Alissa N Antle. 2017. The ethics of doing research with vulnerable populations. Interactions 24, 6 (2017), 74–77.
- Gil Bar-Sela, Lily Atid, Sara Danos, Naomi Gabay, and Ron Epelbaum. 2007. Art therapy improved depression and influenced fatigue levels in cancer patients on chemotherapy. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer 16, 11 (2007), 980–984.
- Paula Maria Barrett. 2000. Treatment of childhood anxiety: Developmental aspects. Clinical Psychology Review 20, 4 (2000), 479–494.
- Aaron T Beck. 1970. Cognitive therapy: Nature and relation to behavior therapy. Behavior therapy 1, 2 (1970), 184–200.
- Aaron T Beck, A John Rush, Brian F Shaw, Gary Emery, Robert J DeRubeis, and Steven D Hollon. 2024. Cognitive Therapy of Depression. Guilford Publications.
- Judith S. Beck. 2020. Cognitive Behavior Therapy: Basics and Beyond. Guilford Publications.
- Staphord Bengesi, Hoda El-Sayed, Md Kamruzzaman Sarker, Yao Houkpati, John Irungu, and Timothy Oladunni. 2024. Advancements in generative AI: A comprehensive review of GANs, GPT, autoencoders, diffusion model, and transformers. IEEe Access 12 (2024), 69812–69837.
- Moti Benita, Raz Kehat, Rotem Zaba, Yael Blumenkranz, Gittit Kessler, Avigail Bar-Sella, and Maya Tamir. 2019. Choosing to regulate emotions: Pursuing emotion goals in autonomy-supportive and controlling contexts. Personality and Social Psychology Bulletin 45, 12 (2019), 1666–1680.
- John T Blackledge and Steven C Hayes. 2001. Emotion regulation in acceptance and commitment therapy. Journal of Clinical Psychology 57, 2 (2001), 243–255.
- Paul Blenkiron. 2005. Stories and analogies in cognitive behaviour therapy: A clinical review. Behavioural and Cognitive Psychotherapy 33, 1 (2005), 45–59.
- Abena Boadi-Agyemang and Minjung Park. 2024. Designing Interactive Agents to Support Emotion Regulation in the Workplace through Guided Art-Making. In Companion of the 2024 ACM/IEEE International Conference on Human-Robot Interaction. 257–262. https://doi.org/10.1145/3610978.3640600
- George A Bonanno and Charles L Burton. 2013. Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspectives on Psychological Science 8, 6 (2013), 591–612.
- Marc A Brackett, Susan E Rivers, Maria R Reyes, and Peter Salovey. 2012. Enhancing academic performance and social and emotional competence with the RULER feeling words curriculum. Learning and Individual Differences 22, 2 (2012), 218–224.
- Virginia Braun and Victoria Clarke. 2006. Using thematic analysis in psychology. Qualitative Research in Psychology 3, 2 (2006), 77–101.
- Robert Brockman, Joseph Ciarrochi, Philip Parker, and Todd Kashdan. 2017. Emotion regulation strategies in daily life: Mindfulness, cognitive reappraisal and emotion suppression. Cognitive Behaviour Therapy 46, 2 (2017), 91–113.
- Eileen Brosnan, Carol Fitzpatrick, John Sharry, and Richard Boyle. 2006. An evaluation of the integrated use of a multimedia storytelling system within a psychotherapy intervention for adolescents.. In CHI ’06 Extended Abstracts on Human Factors in Computing Systems. 598–603. https://doi.org/10.1145/1125451.1125576
- Jason T Buhle, Jennifer A Silvers, Tor D Wager, Richard Lopez, Chukwudi Onyemekwu, Hedy Kober, Jochen Weber, and Kevin N Ochsner. 2014. Cognitive reappraisal of emotion: a meta-analysis of human neuroimaging studies. Cerebral Cortex 24, 11 (2014), 2981–2990.
- Centers for Disease Control and Prevention. 2024. Youth Risk Behavior Survey Data Summary & Trends Report: 2013–2023. https://www.cdc.gov/yrbs/dstr/pdf/YRBS-2023-Data-Summary-Trend-Report.pdf
- Yoon Jeong Cha, Jiongyu Chen, Yasemin Gunal, Qiying Zhu, Mark W Newman, and Sun Young Park. 2025. Collaborative Health-Tracking Technologies for Children and Parents: A Review of Current Studies and Directions for Future Research. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–13. https://doi.org/10.1145/3706598.3713596
- Rosanna Chapman and Bethan Evans. 2020. Using art-based acceptance and commitment therapy (ACT) for an adolescent with anxiety and autism. Clinical Case Studies 19, 6 (2020), 438–455.
- Brian C Chu and Philip C Kendall. 2009. Therapist responsiveness to child engagement: Flexibility within manual-based CBT for anxious youth. Journal of Clinical Psychology 65, 7 (2009), 736–754.
- Eliana C Ciasca, Rita C Ferreira, Carmen LA Santana, Orestes V Forlenza, Glenda D Dos Santos, Paula S Brum, and Paula V Nunes. 2018. Art therapy as an adjuvant treatment for depression in elderly women: a randomized controlled trial. Brazilian Journal of Psychiatry 40 (2018), 256–263.
- Pamela M Cole, Sarah E Martin, and Tracy A Dennis. 2004. Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child Development 75, 2 (2004), 317–333.
- Common Sense Media. 2025. AI Chatbots for Mental Health Support: Risk Assessment. Technical Report. Common Sense Media. https://www.commonsensemedia.org/sites/default/files/featured-content/files/csm-ai-risk-assessment-mental-health-11142025.pdf
- David Coyle and Gavin Doherty. 2009. Clinical evaluations and collaborative design: developing new technologies for mental healthcare interventions. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems. 2051–2060. https://doi.org/10.1145/1518701.1519013
- Nancy A Curry and Tim Kasser. 2005. Can coloring mandalas reduce anxiety?Art Therapy 22, 2 (2005), 81–85.
- Aayushi Dangol, Michele Newman, Robert Wolfe, Jin Ha Lee, Julie A Kientz, Jason Yip, and Caroline Pitt. 2024. Mediating Culture: Cultivating Socio-cultural Understanding of AI in Children through Participatory Design. In Proceedings of the 2024 ACM Designing Interactive Systems Conference. 1805–1822. https://doi.org/10.1145/3643834.3661515
- Claudia Daudén Roquet, Nikki Theofanopoulou, Jaimie L Freeman, Jessica Schleider, James J Gross, Katie Davis, Ellen Townsend, and Petr Slovak. 2022. Exploring Situated & Embodied Support for Youth's Mental Health: Design Opportunities for Interactive Tangible Device. In Proceedings of the 2022 CHI Conference on Human Factors in Computing Systems. 1–16. https://doi.org/10.1145/3491102.3502135
- Katie Davis, Morgan Anderson, Chia-Chen Yang, Sophia Choukas-Bradley, Beth T Bell, and Petr Slovak. 2025. Cross-Disciplinary Perspectives on Youth Digital Well-Being Research: Identifying Notable Developments, Persistent Gaps, and Future Directions. Journal of Adolescent Research 40, 2 (2025), 259–295.
- Kerstin Denecke, Sayan Vaaheesan, and Aaganya Arulnathan. 2020. A mental health chatbot for regulating emotions (SERMO)-concept and usability test. IEEE Transactions on Emerging Topics in Computing 9, 3 (2020), 1170–1182. https://doi.org/10.1109/TETC.2020.2974478
- Xuejun Du, Pengcheng An, Justin Leung, April Li, Linda E Chapman, and Jian Zhao. 2024. DeepThInk: Designing and probing human-AI co-creation in digital art therapy. International Journal of Human-Computer Studies 181 (2024), 103139.
- Kedar Nath Dwivedi. 2006. The Therapeutic Use of Stories. Routledge.
- Jennifer M Eastabrook, Jessica J Flynn, and Tom Hollenstein. 2014. Internalizing symptoms in female adolescents: Associations with emotional awareness and emotion regulation. Journal of Child and Family Studies 23, 3 (2014), 487–496.
- Charles Fage, Charles Consel, Kattalin Etchegoyhen, Anouck Amestoy, Manuel Bouvard, Cécile Mazon, and Hélène Sauzéon. 2019. An emotion regulation app for school inclusion of children with ASD: Design principles and evaluation. Computers & Education 131 (2019), 1–21.
- Alexz Farrall, Jordan Taylor, Ben Ainsworth, and Jason Alexander. 2023. Manifesting Breath: Empirical Evidence for the Integration of Shape-changing Biofeedback-based Artefacts within Digital Mental Health Interventions. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems. 1–14. https://doi.org/10.1145/3544548.3581188
- Kathleen Kara Fitzpatrick, Alison Darcy, and Molly Vierhile. 2017. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): a randomized controlled trial. JMIR Mental Health 4, 2 (2017), e7785. https://doi.org/10.2196/mental.7785
- Daniel Freeman, Jessica C Bird, Bao S Loe, David Kingdon, Helen Startup, David M Clark, Anke Ehlers, Emma Černis, Gail Wingham, Nicole Evans, et al. 2020. The Dunn worry questionnaire and the paranoia worries questionnaire: new assessments of worry. Psychological Medicine 50, 5 (2020), 771–780.
- Robert D Friedberg and Jessica M McClure. 2015. Clinical Practice of Cognitive Therapy with Children and Adolescents: The Nuts and Bolts. Guilford Publications.
- Robert D Friedberg and Laura H Wilt. 2010. Metaphors and stories in cognitive behavioral therapy with children. Journal of Rational-Emotive & Cognitive-Behavior Therapy 28, 2 (2010), 100–113.
- Nadia Garnefski, Vivian Kraaij, and Philip Spinhoven. 2001. Negative life events, cognitive emotion regulation and emotional problems. Personality and Individual differences 30, 8 (2001), 1311–1327.
- Dennis Greenberger and Christine A Padesky. 2015. Mind Over Mood: Change How You Feel by Changing the Way You Think. Vol. 425. Guilford Publications.
- Julien Gross and Harlene Hayne. 1998. Drawing facilitates children's verbal reports of emotionally laden events.Journal of Experimental Psychology: Applied 4, 2 (1998), 163.
- James J Gross. 2008. Emotion Regulation. Handbook of Emotions 3, 3 (2008), 497–513.
- James J Gross. 2015. Emotion regulation: Current status and future prospects. Psychological Inquiry 26, 1 (2015), 1–26.
- Amy G Halberstadt and Kimberly L Eaton. 2002. A meta-analysis of family expressiveness and children's emotion expressiveness and understanding. Marriage & Family Review 34, 1-2 (2002), 35–62.
- Aleesha Hamid, Rabiah Arshad, and Suleman Shahid. 2022. What are you thinking?: Using CBT and Storytelling to Improve Mental Health Among College Students. In Proceedings of the 2022 CHI Conference on Human Factors in Computing Systems. 1–16. https://doi.org/10.1145/3491102.3517603
- Gunnar Harboe and Elaine M Huang. 2015. Real-World Affinity Diagramming Practices: Bridging the Paper-Digital Gap. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems. 95–104. https://doi.org/10.1145/2702123.2702561
- Steven C Hayes, Jason B Luoma, Frank W Bond, Akihiko Masuda, and Jason Lillis. 2006. Acceptance and commitment therapy: Model, processes and outcomes. Behaviour Research and Therapy 44, 1 (2006), 1–25.
- Michael V Heinz, Daniel M Mackin, Brianna M Trudeau, Sukanya Bhattacharya, Yinzhou Wang, Haley A Banta, Abi D Jewett, Abigail J Salzhauer, Tess Z Griffin, and Nicholas C Jacobson. 2025. Randomized trial of a generative AI chatbot for mental health treatment. Nejm Ai 2, 4 (2025), AIoa2400802.
- Clara E Hill, Sarah Knox, Barbara J Thompson, Elizabeth Nutt Williams, Shirley A Hess, and Nicholas Ladany. 2005. Consensual qualitative research: An update.Journal of Counseling Psychology 52, 2 (2005), 196.
- Clara E Hill, Barbara J Thompson, and Elizabeth Nutt Williams. 1997. A guide to conducting consensual qualitative research. The Counseling Psychologist 25, 4 (1997), 517–572.
- Jessica D Hoffmann, Marc A Brackett, Craig S Bailey, and Cynthia J Willner. 2020. Teaching emotion regulation in schools: Translating research into practice with the RULER approach to social and emotional learning.Emotion 20, 1 (2020), 105.
- Emily A Holmes and Andrew Mathews. 2010. Mental imagery in emotion and emotional disorders. Clinical Psychology Review 30, 3 (2010), 349–362.
- Lisa M Horowitz, Jeffrey A Bridge, Stephen J Teach, Elizabeth Ballard, Jennifer Klima, Donald L Rosenstein, Elizabeth A Wharff, Katherine Ginnis, Elizabeth Cannon, Paramjit Joshi, et al. 2012. Ask Suicide-Screening Questions (ASQ): a brief instrument for the pediatric emergency department. Archives of Pediatrics & Adolescent Medicine 166, 12 (2012), 1170–1176.
- Tianqiang Hu, Dajun Zhang, Jinliang Wang, Ritesh Mistry, Guangming Ran, and Xinqiang Wang. 2014. Relation between emotion regulation and mental health: A meta-analysis review. Psychological Reports 114, 2 (2014), 341–362.
- Jui-Wei Huang, Yan-Ming Chen, and Chuang-Wen You. 2024. Music Diary: Using ChatGPT to Craft Interactive Diaries with Emotional Music for Reflection and Sharing Real-life Emotions. In Companion of the 2024 on ACM International Joint Conference on Pervasive and Ubiquitous Computing. 210–213. https://doi.org/10.1145/3675094.3677550
- Yun Huang, Ying Tang, and Yang Wang. 2015. EEmotion Map: A Location-based Mobile Social System for Improving Emotion Awareness and Regulation. In Proceedings of the 18th ACM Conference on Computer Supported Cooperative Work & Social Computing. 130–142. https://doi.org/10.1145/2675133.2675173
- Erin M Ingoldsby. 2010. Review of interventions to improve family engagement and retention in parent and child mental health programs. Journal of Child and Family Studies 19, 5 (2010), 629–645.
- Chen Ji and Katherine Isbister. 2022. AR Fidget: Augmented Reality Experiences that Support Emotion Regulation through Fidgeting. In CHI Conference on Human Factors in Computing Systems Extended Abstracts. 1–4. https://doi.org/10.1145/3491101.3519874
- Lennart Jütte, Ning Wang, Martin Steven, and Bernhard Roth. 2024. Perspectives for generative AI-assisted art therapy for melanoma patients. AI 5, 3 (2024), 1648–1669.
- Manasa Kalanadhabhatta, Adrelys Mateo Santana, Lynnea Mayorga, Tauhidur Rahman, Deepak Ganesan, and Adam Grabell. 2024. Multi-stakeholder Perspectives on Mental Health Screening Tools for Children. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–15. https://doi.org/10.1145/3613904.3642604
- Rachael M Kang and Tera L Reynolds. 2024. “This app said I had severe depression, and now I don't know what to do”: the unintentional harms of mental health applications. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–17. https://doi.org/10.1145/3613904.3642178
- Tero Karras, Samuli Laine, and Timo Aila. 2019. A style-based generator architecture for generative adversarial networks. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition. 4401–4410.
- Philip C Kendall and Muniya S Choudhury. 2003. Children and adolescents in cognitive–behavioral therapy: Some past efforts and current advances, and the challenges in our future. Cognitive Therapy and Research 27, 1 (2003), 89–104.
- Philip C Kendall, Jennifer L Hudson, Elizabeth Gosch, Ellen Flannery-Schroeder, and Cynthia Suveg. 2008. Cognitive-behavioral therapy for anxiety disordered youth: a randomized clinical trial evaluating child and family modalities.Journal of Consulting and Clinical Psychology 76, 2 (2008), 282.
- Taewan Kim, Donghoon Shin, Young-Ho Kim, and Hwajung Hong. 2024. DiaryMate: Understanding User Perceptions and Experience in Human-AI Collaboration for Personal Journaling. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–15. https://doi.org/10.1145/3613904.3642693
- Julie Newman Kingery, Tami L Roblek, Cynthia Suveg, Rachel L Grover, Joel T Sherrill, and R Lindsey Bergman. 2006. They're not just “little adults”: Developmental considerations for implementing cognitive-behavioral therapy with anxious youth. Journal of Cognitive Psychotherapy 20, 3 (2006), 263–273.
- Alexandra Kitson, Alissa N Antle, Sadhbh Kenny, Ashu Adhikari, Kenneth Karthik, Artun Cimensel, and Melissa Chan. 2024. ’I Call Upon a Friend’: Virtual Reality-Based Supports for Cognitive Reappraisal Identified through Co-designing with Adolescents. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–18. https://doi.org/10.1145/3613904.3642723
- Alexandra Kitson, Alissa N Antle, and Petr Slovak. 2023. Co-Designing a Virtual Reality Intervention for Supporting Cognitive Reappraisal Skills Development with Youth. In Proceedings of the 22nd Annual ACM Interaction Design and Children Conference. 14–26. https://doi.org/10.1145/3585088.3589381
- Alexandra Kitson, Petr Slovak, and Alissa N Antle. 2024. Supporting Cognitive Reappraisal With Digital Technology: A Content Analysis and Scoping Review of Challenges, Interventions, and Future Directions. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–17. https://doi.org/10.1145/3613904.3642488
- Faye Kollig, Jessica Pater, Fayika Farhat Nova, and Casey Fiesler. 2025. Fictional Failures and Real-World Lessons: Ethical Speculation Through Design Fiction on Emotional Support Conversational AI. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–15. https://doi.org/10.1145/3706598.3713322
- Richard D Lane and Gary E Schwartz. 1987. Levels of emotional awareness: a cognitive-developmental theory and its application to psychopathology.The American Journal of Psychiatry 144, 2 (1987), 133–143.
- Gwendolyn M Lawson, Meghan E McKenzie, Kimberly D Becker, Lisa Selby, and Sharon A Hoover. 2019. The core components of evidence-based social emotional learning programs. Prevention Science 20, 4 (2019), 457–467.
- Amanda Lazar, Jessica L Feuston, Caroline Edasis, and Anne Marie Piper. 2018. Making as Expression: Informing Design with People with Complex Communication Needs through Art Therapy. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. 1–16. https://doi.org/10.1145/3173574.3173925
- Ronald S Lenkowsky. 1987. Bibliotherapy: A review and analysis of the literature. The Journal of Special Education 21, 2 (1987), 123–132.
- Leigh M Levinson, Nida Itrat Abbasi, Selma Sabanovic, and Hatice Gunes. 2024. Expert insights on robots for safeguarding children: How (not) and why (not)?. In Proceedings of the 23rd Annual ACM Interaction Design and Children Conference. 600–611.
- Rong-Hao Liang, Bin Yu, Mengru Xue, Jun Hu, and Loe MG Feijs. 2018. BioFidget: Biofeedback for Respiration Training Using an Augmented Fidget Spinner. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. 1–12. https://doi.org/10.1145/3173574.3174187
- Marsha Linehan. 1993. Cognitive-Behavioral Treatment of Borderline Personality Disorder. Guilford Press.
- Di Liu, Hanqing Zhou, and Pengcheng An. 2024. " When He Feels Cold, He Goes to the Seahorse"—Blending Generative AI into Multimaterial Storymaking for Family Expressive Arts Therapy. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–21. https://doi.org/10.1145/3613904.3642852
- Long Liu, Junbin Ren, Zeyuan Fan, Chenhui Li, Gaoqi He, Changbo Wang, Yang Gao, and Chen Li. 2025. SandTouch: Empowering Virtual Sand Art in VR with AI Guidance and Emotional Relief. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–21. https://doi.org/10.1145/3706598.3714275
- Cathy A Malchiodi. 2011. Handbook of Art Therapy. Guilford Press.
- Mark Matthews and Gavin Doherty. 2011. My mobile story: therapeutic storytelling for children. In CHI’11 Extended Abstracts on Human Factors in Computing Systems. 2059–2064. https://doi.org/10.1145/1979742.1979860
- Simon McCarthy-Jones, Rebecca Knowles, and Georgina Rowse. 2012. More than words? Hypomanic personality traits, visual imagery and verbal thought in young adults. Consciousness and Cognition 21, 3 (2012), 1375–1381.
- Katie A McLaughlin, Mark L Hatzenbuehler, Douglas S Mennin, and Susan Nolen-Hoeksema. 2011. Emotion dysregulation and adolescent psychopathology: A prospective study. Behaviour Research and Therapy 49, 9 (2011), 544–554.
- Jackie McRae, Christina Smith, Anton Emmanuel, and Suzanne Beeke. 2020. The experiences of individuals with cervical spinal cord injury and their family during post-injury care in non-specialised and specialised units in UK. BMC Health Services Research 20 (2020), 1–11.
- Wim Meeus. 2016. Adolescent psychosocial development: A review of longitudinal models and research.Developmental Psychology 52, 12 (2016), 1969.
- Mental Health America. 2025. Changing Thoughts with an AI Assistant. https://screening.mhanational.org/changing-thoughts-with-an-ai-assistant/. Accessed: 2025-11-19.
- Cade Metz. 2025. Are A.I.Therapy Chatbots Safe to Use?The New York Times (2025). https://www.nytimes.com/2025/11/06/technology/ai-therapy-chatbots-ash.html
- Pardis Miri, Mehul Arora, Aman Malhotra, Robert Flory, Stephanie Hu, Ashley Lowber, Ishan Goyal, Jacqueline Nguyen, John P Hegarty, Marlo D Kohn, et al. 2022. FAR: End-to-End Vibrotactile Distributed System Designed to Facilitate Affect Regulation in Children Diagnosed with Autism Spectrum Disorder Through Slow Breathing. In Proceedings of the 2022 CHI Conference on Human Factors in Computing Systems. 1–20. https://doi.org/10.1145/3491102.3517619
- Pardis Miri, Robert Flory, Andero Uusberg, Heather Culbertson, Richard H Harvey, Agata Kelman, Davis Erik Peper, James J Gross, Katherine Isbister, and Keith Marzullo. 2020. PIV: Placement, Pattern, and Personalization of an Inconspicuous Vibrotactile Breathing Pacer. ACM Transactions on Computer-Human Interaction (TOCHI) 27, 1 (2020), 1–44. https://doi.org/10.1145/3365107
- Paul Montgomery and Kathryn Maunders. 2015. The effectiveness of creative bibliotherapy for internalizing, externalizing, and prosocial behaviors in children: A systematic review. Children and Youth Services Review 55 (2015), 37–47.
- Bruce Moon. 2007. The Role of Metaphor in Art Therapy: Theory, Method, and Experience. Charles C Thomas Publisher.
- Kellen Mrkva, Jacob Westfall, and Leaf Van Boven. 2019. Attention drives emotion: Voluntary visual attention increases perceived emotional intensity. Psychological Science 30, 6 (2019), 942–954.
- Isabel Neto, Yuhan Hu, Filipa Correia, Filipa Rocha, Guy Hoffman, Hugo Nicolau, and Ana Paiva. 2024. Conveying Emotions through Shape-changing to Children with and without Visual Impairment. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–16. https://doi.org/10.1145/3613904.3642525
- Michele Newman, Kaiwen Sun, Ilena B Dalla Gasperina, Grace Y Shin, Matthew Kyle Pedraja, Ritesh Kanchi, Maia B Song, Rannie Li, Jin Ha Lee, and Jason Yip. 2024. " I want it to talk like Darth Vader": Helping Children Construct Creative Self-Efficacy with Generative AI. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–18. https://doi.org/10.1145/3613904.3642492
- Erik C Nook, Stephanie F Sasse, Hilary K Lambert, Katie A McLaughlin, and Leah H Somerville. 2018. The nonlinear development of emotion differentiation: Granular emotional experience is low in adolescence. Psychological Science 29, 8 (2018), 1346–1357.
- William T. O'Donohue and Jane E. Fisher. 2012. Cognitive Behavior Therapy: Core Principles for Practice. John Wiley & Sons.
- Jooyoung Oh, Sooah Jang, Hyunji Kim, and Jae-Jin Kim. 2020. Efficacy of mobile app-based interactive cognitive behavioral therapy using a chatbot for panic disorder. International Journal of Medical Informatics 140 (2020), 104171.
- Pablo E Paredes, Yijun Zhou, Nur Al-Huda Hamdan, Stephanie Balters, Elizabeth Murnane, Wendy Ju, and James A Landay. 2018. Just Breathe: In-Car Interventions for Guided Slow Breathing. Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies 2, 1 (2018), 1–23. https://doi.org/10.1145/3191760
- Pat Pataranutaporn, Chayapatr Archiwaranguprok, Samantha WT Chan, Elizabeth Loftus, and Pattie Maes. 2025. Synthetic Human Memories: AI-Edited Images and Videos Can Implant False Memories and Distort Recollection. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–20. https://doi.org/10.1145/3706598.3713697
- Georgia Pavlopoulou, Susie Chandler, Steve Lukito, Myrofora Kakoulidou, Maciej Matejko, Isabel Jackson, Beta Balwani, Tiegan Boyens, Dorian Poulton, Luke Harvey-Nguyen, et al. 2025. Situating emotion regulation in autism and ADHD through neurodivergent adolescents’ perspectives. Scientific Reports 15, 1 (2025), 37464.
- Tom Percival. 2019. Ruby Finds a Worry. Bloomsbury Publishing USA.
- Mao Theresa Perkins and Daisy Hideko Randolph. 2025. The Enhanced CBT Toolbox for Children and Adolescents: A Practical Workbook for Clinicians, Parents, and Caregivers to Support Emotional Regulation, Mindfulness, Social Skills, and Behavioral Growth. Mao Theresa Perkins.
- Laura Pina, Kael Rowan, Asta Roseway, Paul Johns, Gillian R Hayes, and Mary Czerwinski. 2014. In situ cues for ADHD parenting strategies using mobile technology. In Proceedings of the 8th International Conference on Pervasive Computing Technologies for Healthcare. 17–24. https://doi.org/10.4108/icst.pervasivehealth.2014.254958
- Abigail E Pine, Mary G Baumann, Gabriella Modugno, and Bruce E Compas. 2024. Parental involvement in adolescent psychological interventions: a meta-analysis. Clinical Child and Family Psychology Review 27, 3 (2024), 1–20.
- Aditya Ramesh, Mikhail Pavlov, Gabriel Goh, Scott Gray, Chelsea Voss, Alec Radford, Mark Chen, and Ilya Sutskever. 2021. Zero-shot text-to-image generation. In International Conference on Machine Learning. PMLR, 8821–8831.
- Laura P Richardson, Elizabeth McCauley, David C Grossman, Carolyn A McCarty, Julie Richards, Joan E Russo, Carol Rockhill, and Wayne Katon. 2010. Evaluation of the Patient Health Questionnaire-9 Item for detecting major depression among adolescents. Pediatrics 126, 6 (2010), 1117–1123.
- Michael B. Robb and Supreet Mann. 2025. Talk, Trust, and Trade-Offs: How and Why Teens Use AI Companions. Technical Report. Common Sense Media, San Francisco, CA. https://www.commonsensemedia.org/sites/default/files/research/report/talk-trust-and-trade-offs_2025_web.pdf
- Guy Roth, Maarten Vansteenkiste, and Richard M Ryan. 2019. Integrative emotion regulation: Process and development from a self-determination theory perspective. Development and Psychopathology 31, 3 (2019), 945–956.
- Kimiko Ryokai, Hayes Raffle, and Robert Kowalski. 2012. StoryFaces: pretend-play with ebooks to support social-emotional storytelling. In Proceedings of the 11th International Conference on Interaction Design and Children. 125–133. https://doi.org/10.1145/2307096.2307111
- Book Sadprasid, Anne Mei, Alex Mariakakis, Scott Bateman, and Fanny Chevalier. 2024. Leveraging Idle Games to Incentivize Intermittent and Frequent Practice of Deep Breathing. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–17.
- Herman Saksono and Andrea G Parker. 2017. Reflective Informatics Through Family Storytelling: Self-discovering Physical Activity Predictors. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems. 5232–5244. https://doi.org/10.1145/3025453.3025651
- Pedro Sanches, Axel Janson, Pavel Karpashevich, Camille Nadal, Chengcheng Qu, Claudia Daudén Roquet, Muhammad Umair, Charles Windlin, Gavin Doherty, Kristina Höök, et al. 2019. HCI and Affective Health: Taking stock of a decade of studies and charting future research directions. In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems. 1–17. https://doi.org/10.1145/3290605.3300475
- Angela Scarpa and Nuri M Reyes. 2011. Improving emotion regulation with CBT in young children with high functioning autism spectrum disorders: A pilot study. Behavioural and Cognitive Psychotherapy 39, 4 (2011), 495–500.
- Jessica Schroeder, Chelsey Wilkes, Kael Rowan, Arturo Toledo, Ann Paradiso, Mary Czerwinski, Gloria Mark, and Marsha M Linehan. 2018. Pocket Skills: A Conversational Mobile Web App To Support Dialectical Behavioral Therapy. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. 1–15. https://doi.org/10.1145/3173574.3173972
- Susanne Schweizer, Ian H Gotlib, and Sarah-Jayne Blakemore. 2020. The role of affective control in emotion regulation during adolescence.Emotion 20, 1 (2020), 80.
- Forrest Scogin, Jerry Bynum, Gretchen Stephens, and Sharon Calhoon. 1990. Efficacy of self-administered treatment programs: Meta-analytic review.Professional Psychology: Research and Practice 21, 1 (1990), 42.
- Laura D Seligman and Thomas H Ollendick. 2011. Cognitive behavioral therapy for anxiety disorders in youth. Child and Adolescent Psychiatric Clinics of North America 20, 2 (2011), 217.
- Woosuk Seo, Chanmo Yang, and Young-Ho Kim. 2024. ChaCha: Leveraging Large Language Models to Prompt Children to Share Their Emotions about Personal Events. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–20. https://doi.org/10.1145/3613904.3642152
- Jocelyn J Shen, Jennifer King Chen, Leah Findlater, and Griffin Dietz Smith. 2025. eaSEL: Promoting Social-Emotional Learning and Parent-Child Interaction through AI-Mediated Content Consumption. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–18. https://doi.org/10.1145/3706598.3713405
- Yan Shi, Lidan Gong, Yiwen Lu, Lijuan Liu, Chao Zhang, Shujun Zhang, Longfei Wang, and Shan Zhou. 2025. " I Need Your Help!": Facilitating Psychological Communication Between Left-Behind Children and Their Parents with an AI-Powered Sandbox. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–19. https://doi.org/10.1145/3706598.3713660
- Jennifer S Silk, Gede Pramana, Stefanie L Sequeira, Oliver Lindhiem, Philip C Kendall, Dana Rosen, and Bambang Parmanto. 2020. Using a smartphone app and clinician portal to enhance brief cognitive behavioral therapy for childhood anxiety disorders. Behavior Therapy 51, 1 (2020), 69–84.
- Petr Slovak, Alissa Antle, Nikki Theofanopoulou, Claudia Daudén Roquet, James Gross, and Katherine Isbister. 2023. Designing for Emotion Regulation Interventions: An Agenda for HCI Theory and Research. ACM Transactions on Computer-Human Interaction 30, 1 (2023), 1–51. https://doi.org/0.1145/3569898
- Petr Slovak and Sean A Munson. 2024. HCI Contributions in Mental Health: A Modular Framework to Guide Psychosocial Intervention Design. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–21. https://doi.org/10.1145/3613904.3642624
- Petr Slovák, Kael Rowan, Christopher Frauenberger, Ran Gilad-Bachrach, Mia Doces, Brian Smith, Rachel Kamb, and Geraldine Fitzpatrick. 2016. Scaffolding the scaffolding: Supporting children's social-emotional learning at home. In Proceedings of the 19th ACM Conference on Computer-Supported Cooperative Work & Social Computing. 1751–1765. https://doi.org/10.1145/2818048.2820007
- Jose Luis Soler-Dominguez, Samuel Navas-Medrano, and Patricia Pons. 2024. ARCADIA: A Gamified Mixed Reality System for Emotional Regulation and Self-Compassion. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–17. https://doi.org/10.1145/3613904.3642123
- Michael A Southam-Gerow, Adriana Rodriguez, Bruce F Chorpita, and Eric L Daleiden. 2012. Dissemination and implementation of evidence based treatments for youth: Challenges and recommendations.Professional Psychology: Research and Practice 43, 5 (2012), 527.
- David Spiegel, Cathy Malchiodi, Amy Backos, and Kate Collie. 2006. Art therapy for combat-related PTSD: Recommendations for research and practice. Art Therapy 23, 4 (2006), 157–164.
- Robert L Spitzer, Kurt Kroenke, Janet BW Williams, and Bernd Löwe. 2006. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine 166, 10 (2006), 1092–1097.
- Paul Stallard. 2019. Think good, feel good: A cognitive behavioural therapy workbook for children and young people. John Wiley & Sons.
- Jingjing Sun, Jingyi Yang, Guyue Zhou, Yucheng Jin, and Jiangtao Gong. 2024. Understanding Human-AI Collaboration in Music Therapy Through Co-Design with Therapists. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–21. https://doi.org/10.1145/3613904.3642764
- Cynthia Suveg, Erica Sood, Jonathan S Comer, and Philip C Kendall. 2009. Changes in emotion regulation following cognitive-behavioral therapy for anxious youth. Journal of Clinical Child & Adolescent Psychology 38, 3 (2009), 390–401.
- Yilin Tang, Liuqing Chen, Ziyu Chen, Wenkai Chen, Yu Cai, Yao Du, Fan Yang, and Lingyun Sun. 2024. EmoEden: Applying Generative Artificial Intelligence to Emotional Learning for Children with High-Function Autism. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–20. https://doi.org/10.1145/3613904.3642899
- Joanne Tarver, David Daley, Joanna Lockwood, and Kapil Sayal. 2014. Are self-directed parenting interventions sufficient for externalising behaviour problems in childhood? A systematic review and meta-analysis. European Child & Adolescent Psychiatry 23, 12 (2014), 1123–1137.
- Nikki Theofanopoulou, Alissa N Antle, and Petr Slovak. 2024. " They Don't Come With a Handbook": Exploring Design Opportunities for Supporting Parent-Child Interaction around Emotions in the Family Context. Proceedings of the ACM on Human-computer Interaction 8, CSCW1 (2024), 1–33. https://doi.org/10.1145/3637409
- Nikki Theofanopoulou, Katherine Isbister, Julian Edbrooke-Childs, and Petr Slovák. 2019. A smart toy intervention to promote emotion regulation in middle childhood: feasibility study. JMIR Mental Health 6, 8 (2019), e14029.
- Anja Thieme, Jayne Wallace, Paula Johnson, John McCarthy, Siân Lindley, Peter Wright, Patrick Olivier, and Thomas D Meyer. 2013. Design to promote mindfulness practice and sense of self for vulnerable women in secure hospital services. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems. 2647–2656.
- Theresa Van Lith. 2016. Art therapy in mental health: A systematic review of approaches and practices. The Arts in Psychotherapy 47 (2016), 9–22.
- Cati Vaucelle, Leonardo Bonanni, and Hiroshi Ishii. 2009. Design of haptic interfaces for therapy. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems. 467–470. https://doi.org/10.1145/1518701.1518776
- Marjan Verstappen, Paula Gardner, Dora Poon, and Tim Bettridge. 2014. Off the couch and out of the hospital, mobile applications for acceptance and commitment therapy. In Proceedings of the 16th International Conference on Human-Computer Interaction with Mobile Devices & Services. 431–434. https://doi.org/10.1145/2628363.2633573
- Preeti Vyas, Unma Mayur Desai, Karin Yamakawa, and Karon Maclean. 2023. A Descriptive Analysis of a Formative Decade of Research in Affective Haptic System Design. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems. 1–23. https://doi.org/10.1145/3544548.3580735
- Torben Wallbaum, Andrii Matviienko, Swamy Ananthanarayan, Thomas Olsson, Wilko Heuten, and Susanne CJ Boll. 2018. Supporting Communication between Grandparents and Grandchildren through Tangible Storytelling Systems. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. 1–12. https://doi.org/10.1145/3173574.3174124
- Shun-Yu Wang, Chia-Yu Cheng, Shu-Meng Huang, Weng Io Chan, Yu-Hsuan Huang, and Jhih-Wei Lin. 2023. Breathero: Not Another Slow Breathing Game—Exploring Faster-Paced VR Breathing Exercise Games. In Extended Abstracts of the 2023 CHI Conference on Human Factors in Computing Systems. 1–7. https://doi.org/10.1145/3544549.3583829
- Roger P Weissberg, Joseph A Durlak, Celene E Domitrovich, and Thomas P Gullotta. 2015. Social and emotional learning: Past, present, and future. (2015).
- Gloria Willcox. 1982. The feeling wheel: A tool for expanding awareness of emotions and increasing spontaneity and intimacy. Transactional Analysis Journal 12, 4 (1982), 274–276.
- Wisconsin Office of Children's Mental Health. n.d.. Feelings Thermometer. https://children.wi.gov/Pages/FeelingsThermometer.aspx Accessed: 2025-08-01.
- Yu Xing, Sravanti Vadrevu, and Ji Youn Shin. 2024. Design Opportunities for International Students’ Mental Health Management: An Interview Study with University Counselors. In Companion Publication of the 2024 Conference on Computer-Supported Cooperative Work and Social Computing. 330–335.
- JungKyoon Yoon, Shuran Li, and Yu Hao. 2022. Design-mediated positive emotion regulation: The development of an interactive device that supports daily practice of positive mental time traveling. International Journal of Human–Computer Interaction 38, 5 (2022), 432–446.
- Judith Young and P Fanselow-Brown. 1996. Cognitive behaviour therapy for anxiety: practical tips for using it with children. In Clinical Psychology Forum, Vol. 91. 19–21.
- Benjamin Zablotsky, Amanda E Ng, Lindsey I Black, Jonaki Bose, Jessica R Jones, Aaron K Maitland, and Stephen J Blumberg. 2024. Perceived social and emotional support among teenagers: United States, July 2021–December 2022. In National Health Statistics Reports [Internet]. National Center for Health Statistics (US).
- Janice Zeman, Michael Cassano, Carisa Perry-Parrish, and Sheri Stegall. 2006. Emotion regulation in children and adolescents. Journal of Developmental & Behavioral Pediatrics 27, 2 (2006), 155–168.
- Yijun Zhao, Zhengke Li, Yicheng Wang, Xueyan Cai, Xiaojing Zhou, Yifan Yan, Kecheng Jin, Shiying Ding, Yilin Shao, Jiacheng Cao, et al. 2025. DreamDirector: Designing a Generative AI System to Aid Therapists in Treating Clients’ Nightmares. In Proceedings of the 30th International Conference on Intelligent User Interfaces. 553–578. https://doi.org/10.1145/3708359.3712078
- Xi Zheng, Zhuoyang Li, Xinning Gui, and Yuhan Luo. 2025. Customizing Emotional Support: How Do Individuals Construct and Interact With LLM-Powered Chatbots. In Proceedings of the 2025 CHI Conference on Human Factors in Computing Systems. 1–20. https://doi.org/10.1145/3706598.3713453
- Hanqing Zhou, Anastasia Nikolova, and Pengcheng An. 2024. ’My lollipop dropped...’–Probing Design Opportunities for SEL Agents through Children's Peer Co-Creation of Social-Emotional Stories. In Extended Abstracts of the CHI Conference on Human Factors in Computing Systems. 1–8. https://doi.org/10.1145/3613905.3651867
- Peter Zimmermann and Alexandra Iwanski. 2014. Emotion regulation from early adolescence to emerging adulthood and middle adulthood: Age differences, gender differences, and emotion-specific developmental variations. International Journal of Behavioral Development 38, 2 (2014), 182–194.
- Joseph E Zins and Maurice J Elias. 2007. Social and emotional learning: Promoting the development of all students. Journal of Educational and Psychological Consultation 17, 2-3 (2007), 233–255.
- Annuska Zolyomi and Jaime Snyder. 2024. An Emotion Translator: Speculative Design By Neurodiverse Dyads. In Proceedings of the 2024 CHI Conference on Human Factors in Computing Systems. 1–18. https://doi.org/10.1145/3613904.3642210
- Ania Zubala, Alison Pease, Kacper Lyszkiewicz, and Simon Hackett. 2025. Art psychotherapy meets creative AI: an integrative review positioning the role of creative AI in art therapy process. Frontiers in Psychology 16 (2025), 1548396.
Footnote

This work is licensed under a Creative Commons Attribution 4.0 International License.
CHI '26, Barcelona, Spain
© 2026 Copyright held by the owner/author(s).
ACM ISBN 979-8-4007-2278-3/26/04.
DOI: https://doi.org/10.1145/3772318.3790909